

Real-time active MR-tracking of metallic stylets in MR-guided radiation therapy
- PMID: 24903165
- PMCID: PMC4257908
- DOI: 10.1002/mrm.25300
Real-time active MR-tracking of metallic stylets in MR-guided radiation therapy
Abstract
Purpose: To develop an active MR-tracking system to guide placement of metallic devices for radiation therapy.
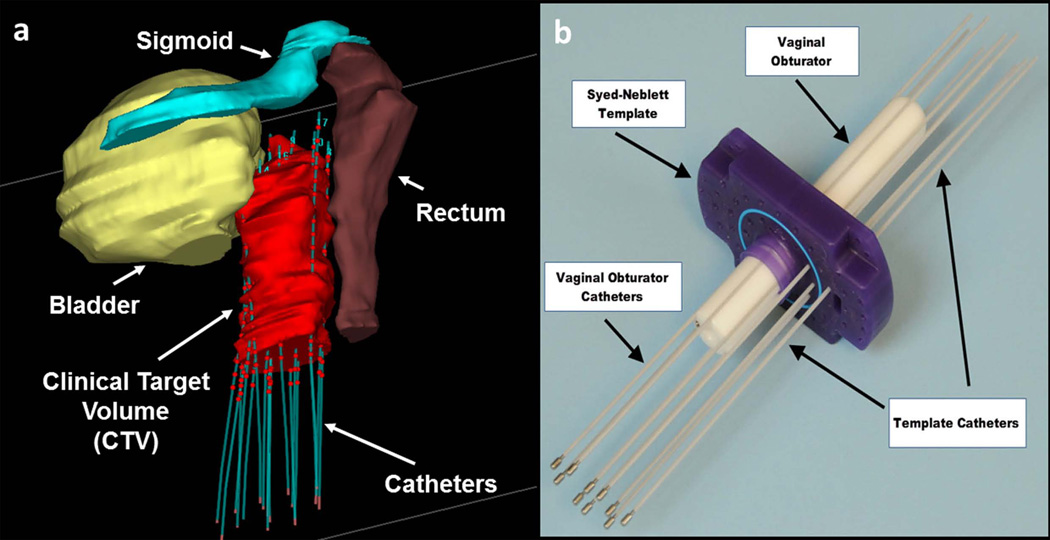
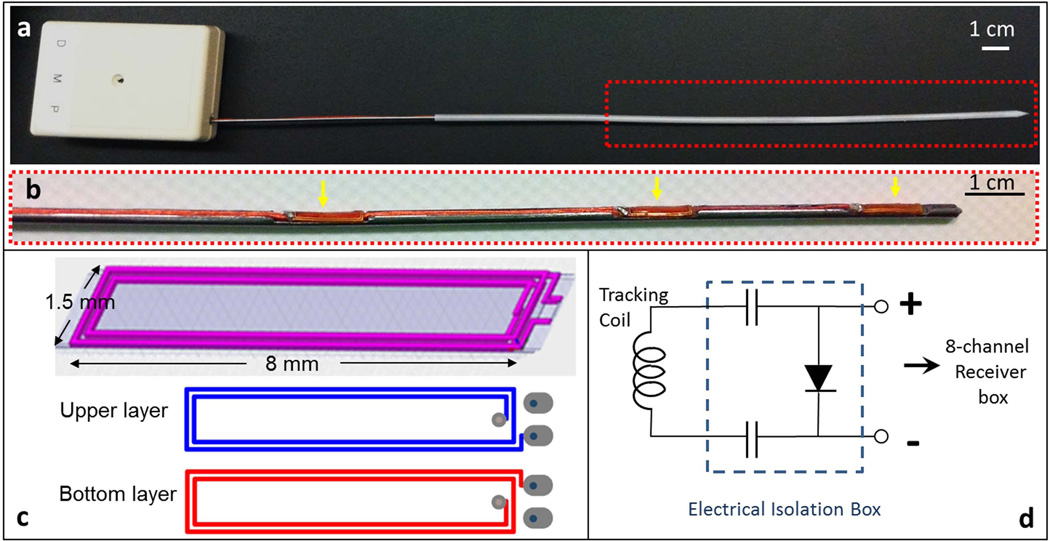
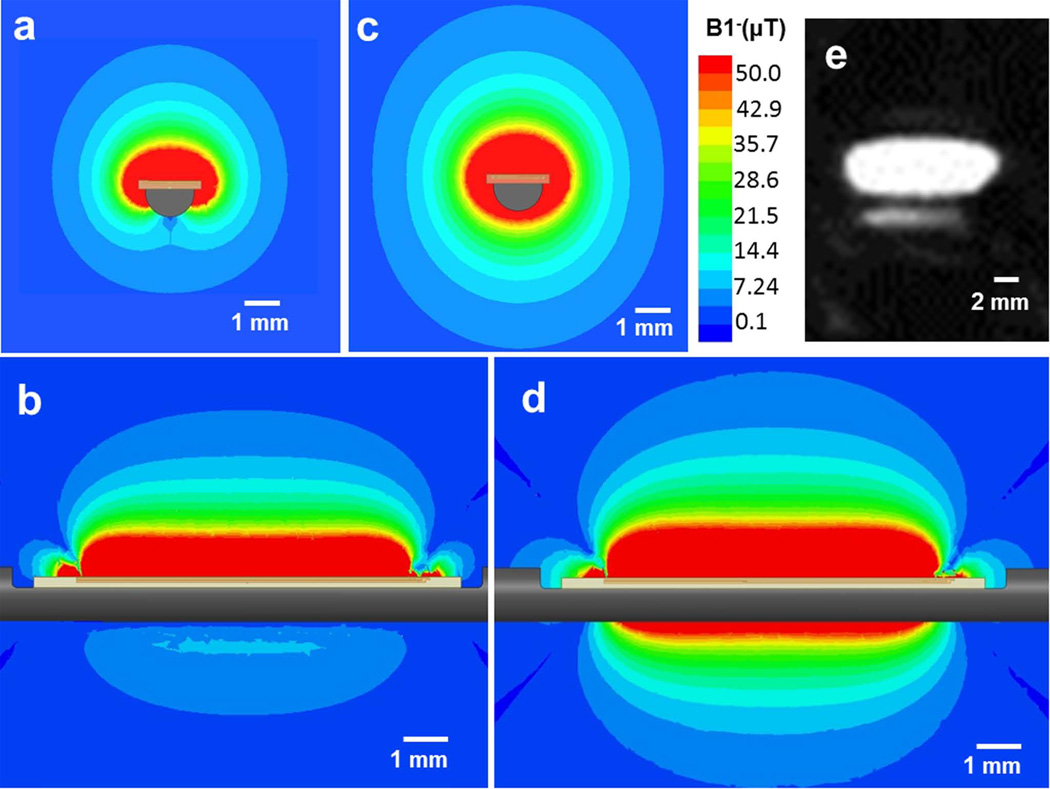
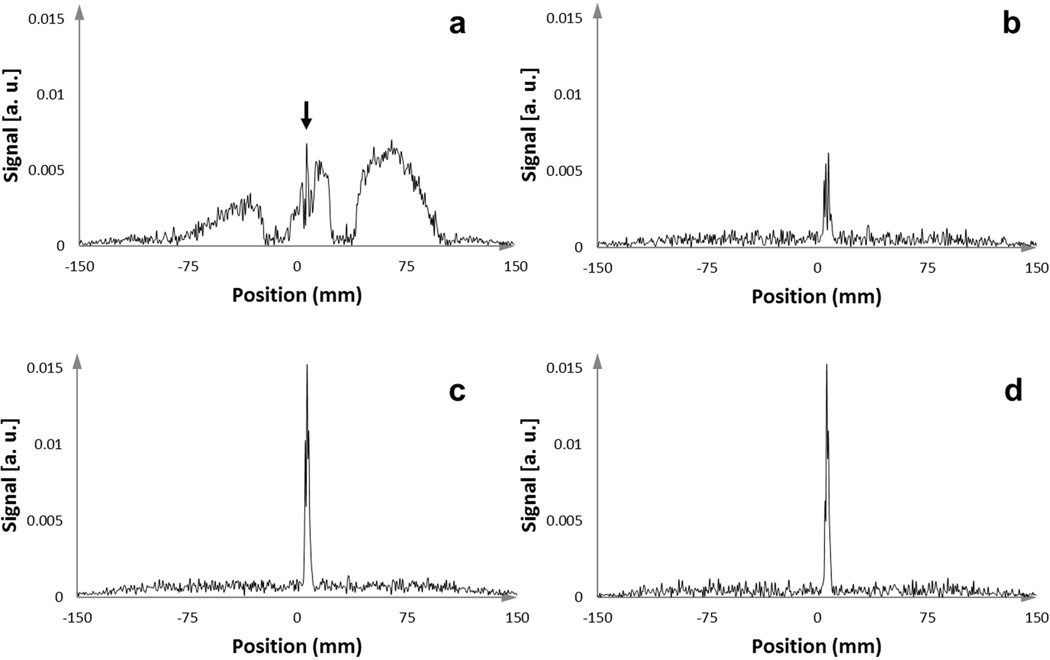
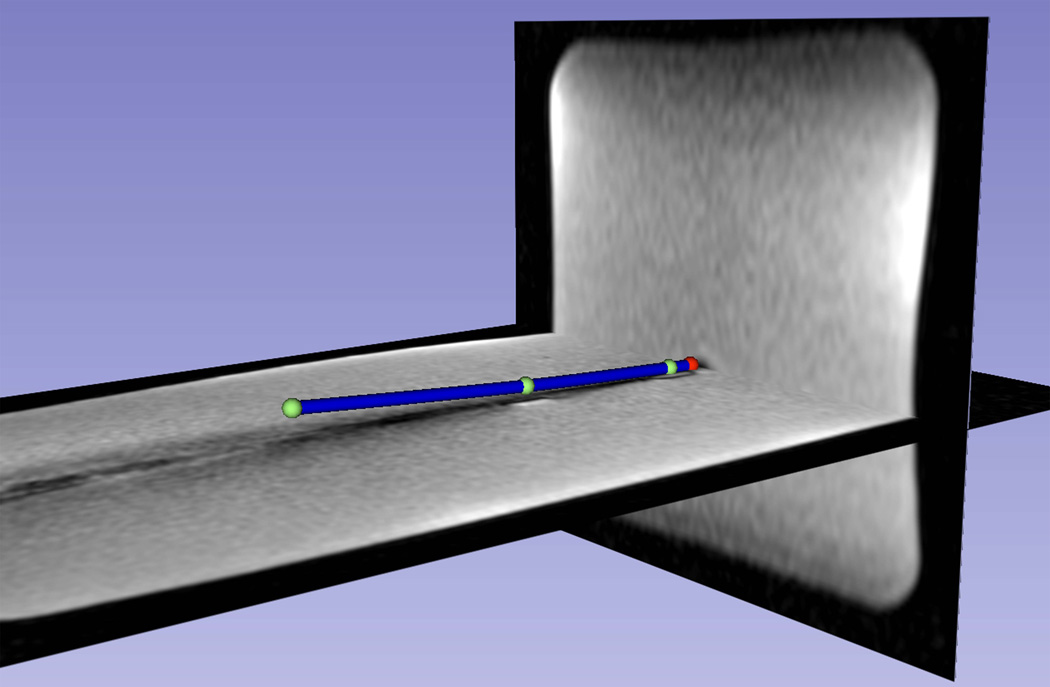
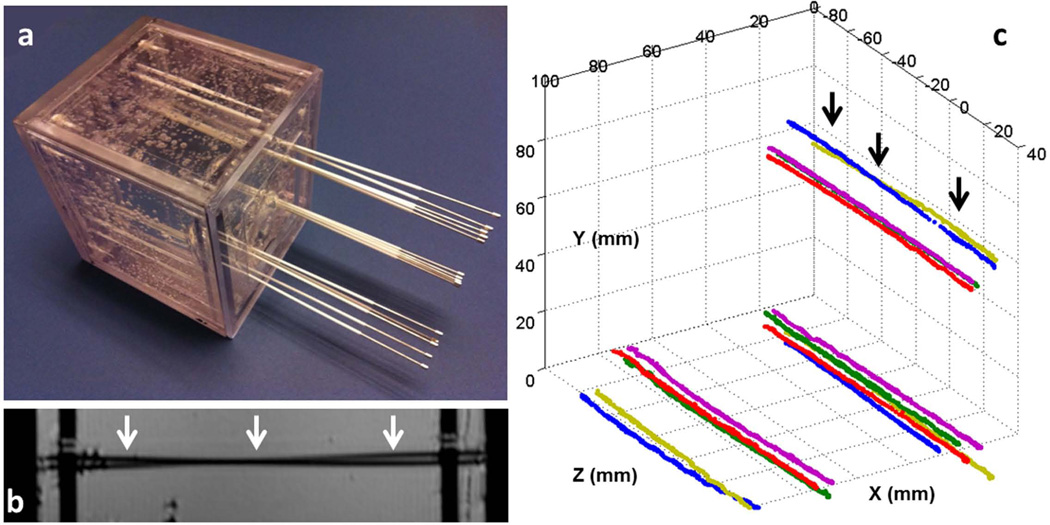
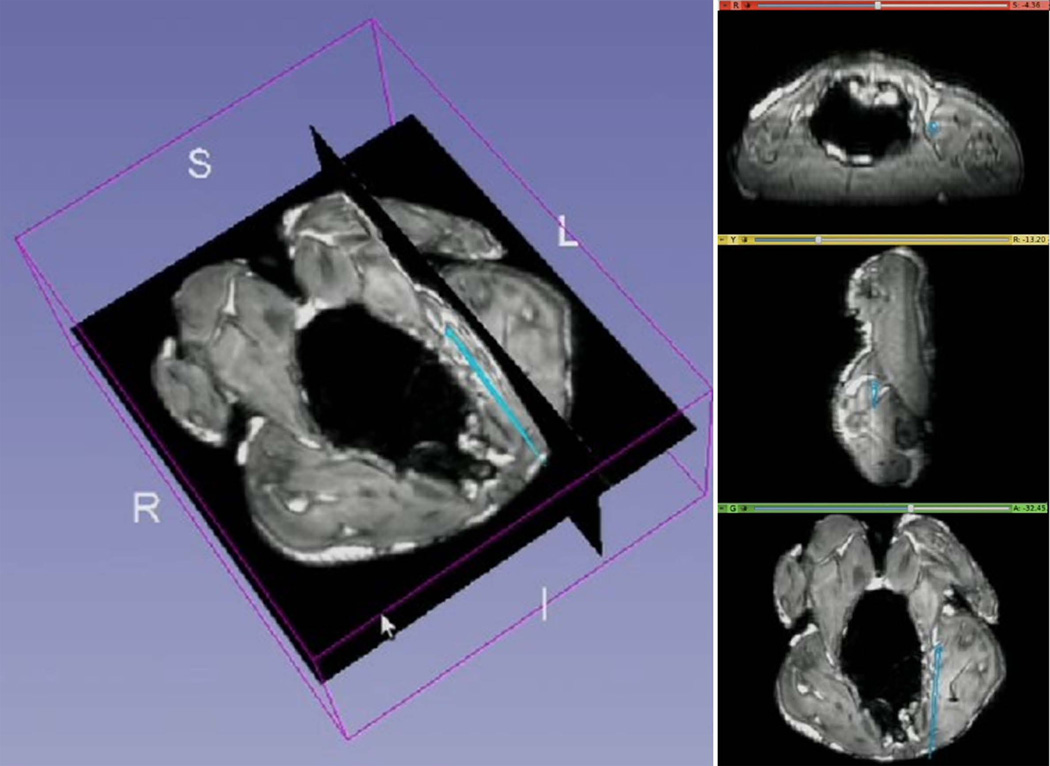
Methods: An actively tracked metallic stylet for brachytherapy was constructed by adding printed-circuit micro-coils to a commercial stylet. The coil design was optimized by electromagnetic simulation, and has a radio-frequency lobe pattern extending ∼5 mm beyond the strong B0 inhomogeneity region near the metal surface. An MR-tracking sequence with phase-field dithering was used to overcome residual effects of B0 and B1 inhomogeneities caused by the metal, as well as from inductive coupling to surrounding metallic stylets. The tracking system was integrated with a graphical workstation for real-time visualization. The 3 Tesla MRI catheter-insertion procedures were tested in phantoms and ex vivo animal tissue, and then performed in three patients during interstitial brachytherapy.
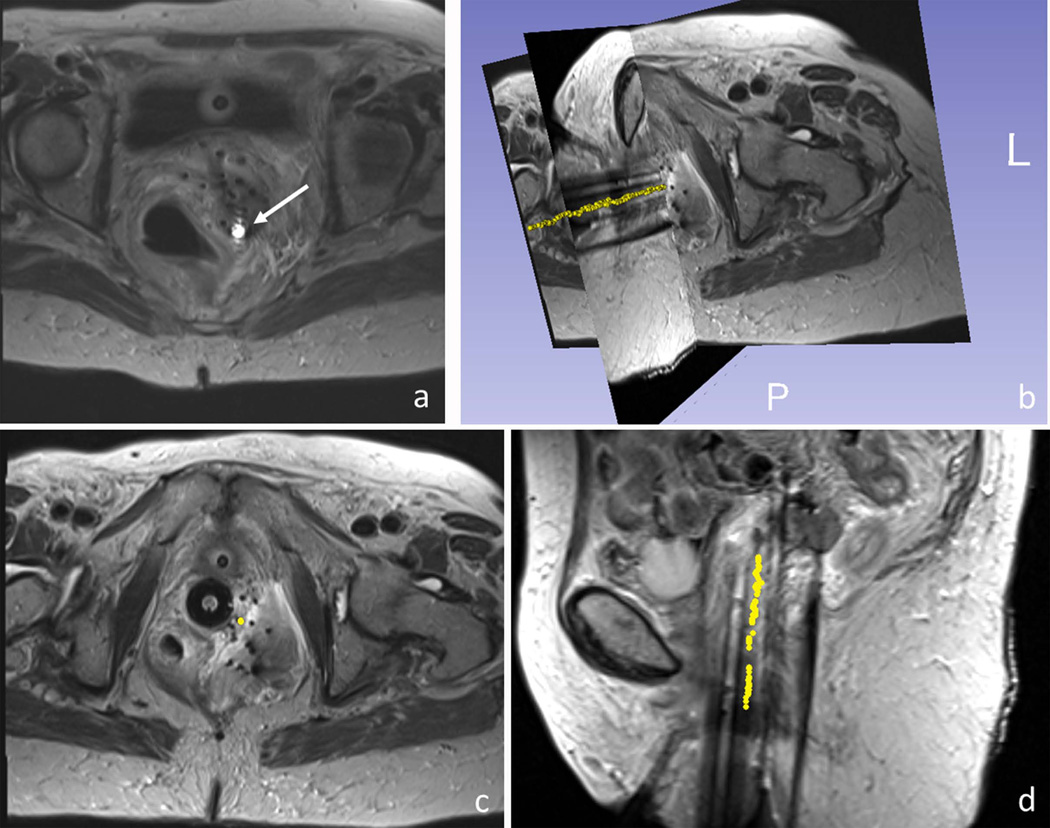
Results: The tracking system provided high-resolution (0.6 × 0.6 × 0.6 mm(3) ) and rapid (16 to 40 frames per second, with three to one phase-field dithering directions) catheter localization in phantoms, animals, and three gynecologic cancer patients.
Conclusion: This is the first demonstration of active tracking of the shaft of metallic stylet in MR-guided brachytherapy. It holds the promise of assisting physicians to achieve better targeting and improving outcomes in interstitial brachytherapy.
Keywords: active MR-tracking; metallic device; phase-field dithering; radiation therapy.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Cancer facts and figures 2013. 250 Williams Street, NW, Atlanta, GA A 30303-1002: Corporate Center: American Cancer Society Inc.;
-
- Han K, Milosevic M, Fyles A, Pintilie M, Viswanathan AN. Trends in the utilization of brachytherapy in cervical cancer in the United States. International journal of radiation oncology, biology, physics. 2013;87(1):111–119. - PubMed
-
- Viswanathan AN, Cormack R, Holloway CL, Tanaka C, O'Farrell D, Devlin PM, Tempany C. Magnetic resonance-guided interstitial therapy for vaginal recurrence of endometrial cancer. International journal of radiation oncology, biology, physics. 2006;66(1):91–99. - PubMed
-
- Viswanathan AN, Szymonifka J, Tempany-Afdhal CM, O'Farrell DA, Cormack RA. A prospective trial of real-time magnetic resonance-guided catheter placement in interstitial gynecologic brachytherapy. Brachytherapy. 2013;12(3):240–247. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
