

GFAP out-performs S100β in detecting traumatic intracranial lesions on computed tomography in trauma patients with mild traumatic brain injury and those with extracranial lesions
- PMID: 24903744
- PMCID: PMC4224051
- DOI: 10.1089/neu.2013.3245
GFAP out-performs S100β in detecting traumatic intracranial lesions on computed tomography in trauma patients with mild traumatic brain injury and those with extracranial lesions
Abstract
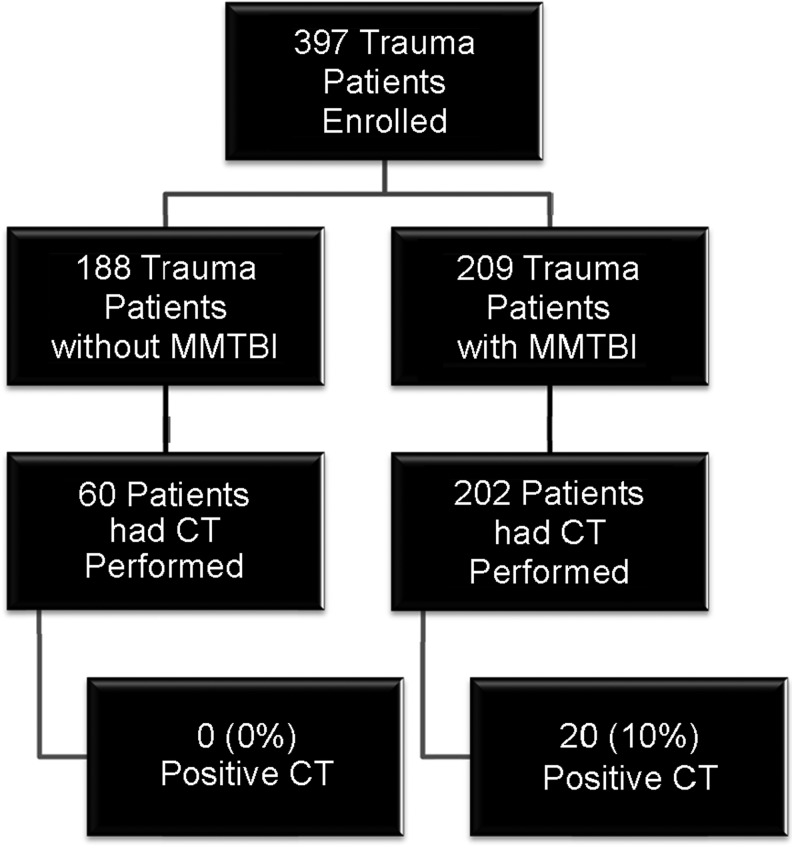
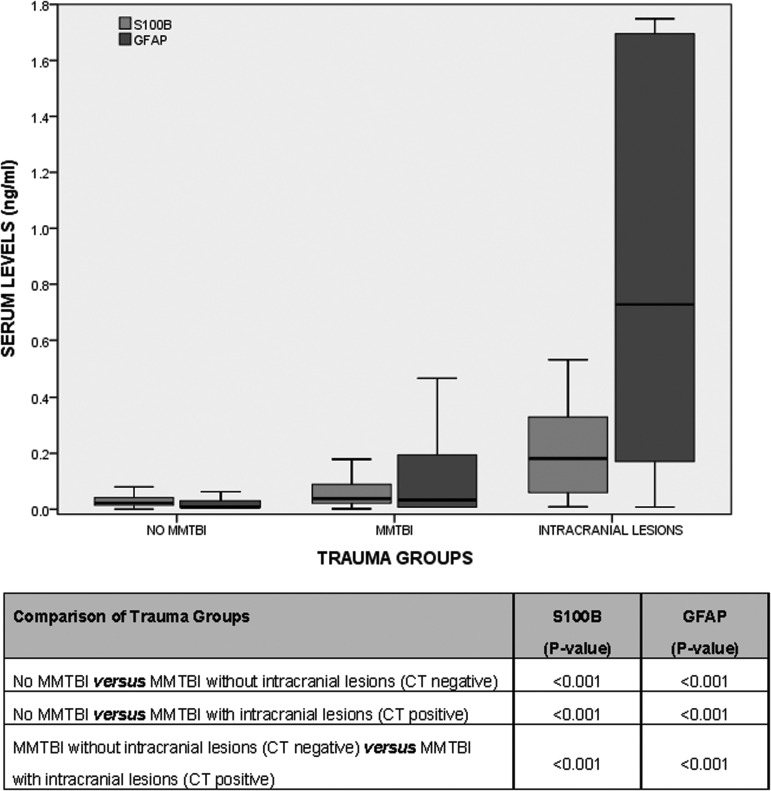
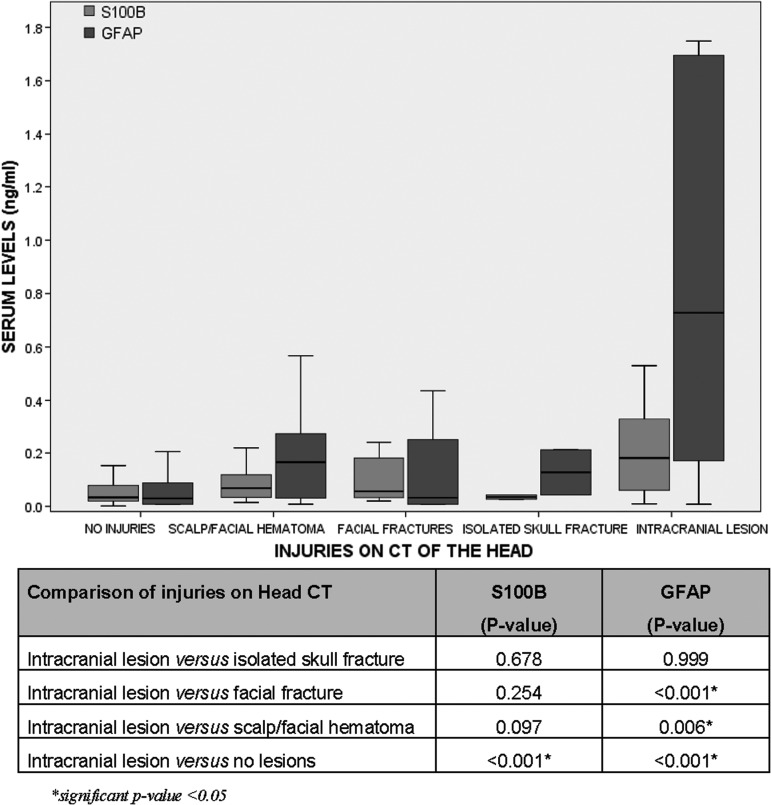
Both glial fibrillary acidic protein (GFAP) and S100β are found in glial cells and are released into serum following a traumatic brain injury (TBI), however, the clinical utility of S100β as a biomarker has been questioned because of its release from bone. This study examined the ability of GFAP and S100β to detect intracranial lesions on computed tomography (CT) in trauma patients and also assessed biomarker performance in patients with fractures and extracranial injuries on head CT. This prospective cohort study enrolled a convenience sample of adult trauma patients at a Level I trauma center with and without mild or moderate traumatic brain injury (MMTBI). Serum samples were obtained within 4 h of injury. The primary outcome was the presence of traumatic intracranial lesions on CT scan. There were 397 general trauma patients enrolled: 209 (53%) had a MMTBI and 188 (47%) had trauma without MMTBI. Of the 262 patients with a head CT, 20 (8%) had intracranial lesions. There were 137 (35%) trauma patients who sustained extracranial fractures below the head to the torso and extremities. Levels of S100β were significantly higher in patients with fractures, compared with those without fractures (p<0.001) whether MMTBI was present or not. However, GFAP levels were not significantly affected by the presence of fractures (p>0.05). The area under the receiver operating characteristics curve (AUC) for predicting intracranial lesions on CT for GFAP was 0.84 (0.73-0.95) and for S100β was 0.78 (0.67-0.89). However, in the presence of extracranial fractures, the AUC for GFAP increased to 0.93 (0.86-1.00) and for S100β decreased to 0.75 (0.61-0.88). In a general trauma population, GFAP out-performed S100β in detecting intracranial CT lesions, particularly in the setting of extracranial fractures.
Keywords: S100β; computed tomography (CT); fractures; glial fibrillary acidic protein (GFAP); mild traumatic brain injury/concussion.
Figures



References
-
- Kochanek P.M., Berger R.P., Bayr H., Wagner A.K., Jenkins L.W., and Clark R.S. (2008) Biomarkers of primary and evolving damage in traumatic and ischemic brain injury: diagnosis, prognosis, probing mechanisms, and therapeutic decision making Curr. Opin. Crit. Care 14, 135–141 - PubMed
-
- Papa L. (2012) Exploring the role of biomarkers for the diagnosis and management of traumatic brain injury patients, in: Poteomics - Human Diseases and Protein Functions. Man T.K. and Flores R.J. (eds). In Tech Open Access Publisher
-
- Xiong H., Liang W.L., and Wu X.R. (2000) [Pathophysiological alterations in cultured astrocytes exposed to hypoxia/reoxygenation]. Sheng Li Ke Xue Jin Zhan 31, 217–221 - PubMed
-
- Ingebrigtsen T., Romner B., Marup-Jensen S., Dons M., Lundqvist C., Bellner J., Alling C., and Borgesen S.E. (2000) The clinical value of serum S-100 protein measurements in minor head injury: a Scandinavian multicentre study. Brain Inj. 14, 1047–1055 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
