

Is right ventricular mid-septal pacing superior to apical pacing in patients with high degree atrio-ventricular block and moderately depressed left ventricular function?
- PMID: 24903987
- PMCID: PMC4116854
- DOI: 10.1631/jzus.B1400034
Is right ventricular mid-septal pacing superior to apical pacing in patients with high degree atrio-ventricular block and moderately depressed left ventricular function?
Abstract
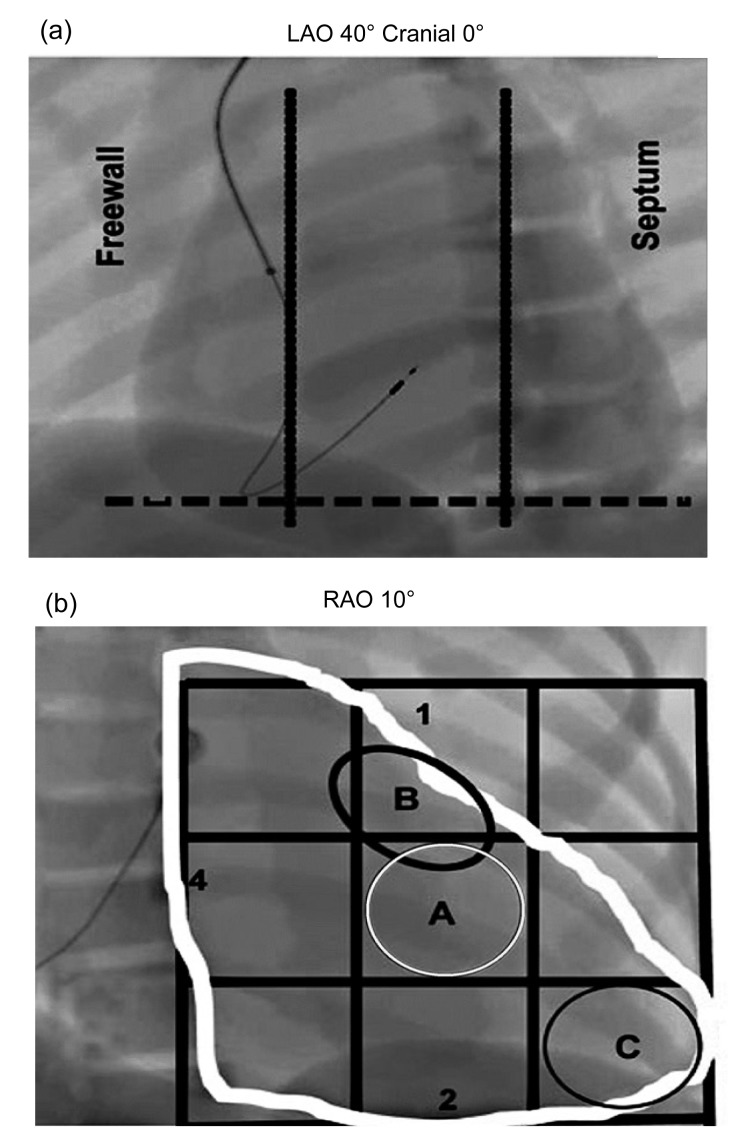
Objective: We are aimed to investigate whether right ventricular mid-septal pacing (RVMSP) is superior to conventional right ventricular apical pacing (RVAP) in improving clinical functional capacity and left ventricular ejection fraction (LVEF) for patients with high-degree atrio-ventricular block and moderately depressed left ventricle (LV) function.
Methods: Ninety-two patients with high-degree atrio-ventricular block and moderately reduced LVEF (ranging from 35% to 50%) were randomly allocated to RVMSP (n=45) and RVAP (n=47). New York Heart Association (NYHA) functional class, echocardiographic LVEF, and distance during a 6-min walk test (6MWT) were determined at 18 months after pacemaker implantation. Serum levels of N-terminal pro-brain natriuretic peptide (NT-proBNP) were measured using an enzyme-linked immunosorbent assay (ELISA) kit.
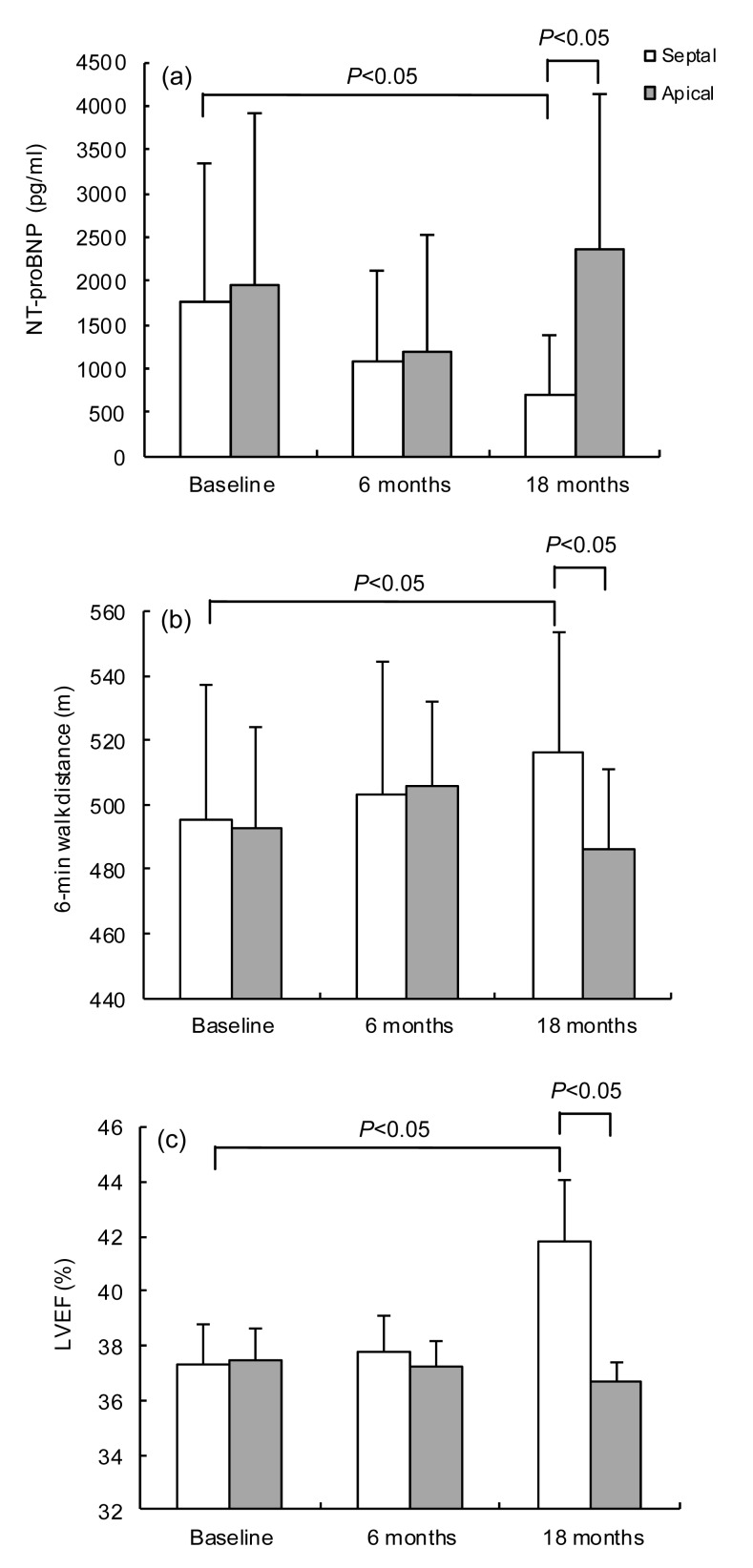
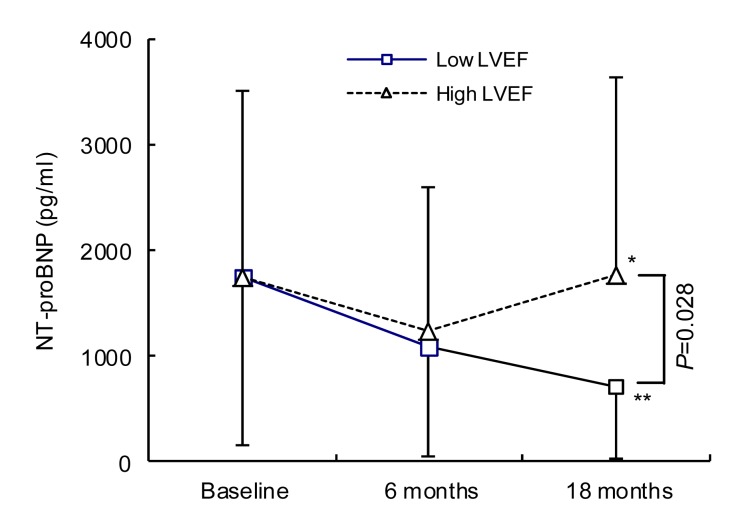
Results: Compared with baseline, NYHA functional class remained unchanged at 18 months, distance during 6MWT (485 m vs. 517 m) and LVEF (36.7% vs. 41.8%) were increased, but BNP levels were reduced (2352 pg/ml vs. 710 pg/ml) in the RVMSP group compared with those in the RVAP group, especially in patients with LVEF 35%-40% (for all comparisons, P<0.05). However, clinical function capacity and LV function measurements were not significantly changed in patients with RVAP, despite the pacing measurements being similar in both groups, such as R-wave amplitude and capture threshold.
Conclusions: RVMSP provides a better clinical utility, compared with RVAP, in patients with high-degree atrioventricular block and moderately depressed LV function whose LVEF levels ranged from 35% to 40%.
Keywords: Apical pacing; Impaired heart function; Mid-septal pacing.
Conflict of interest statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study. Additional informed consent was obtained from all patients for which identifying information is included in this article.
Figures
References
-
- Chiladakis JA, Koutsogiannis N, Kalogeropoulos A, et al. Permanent and atrial-synchronized ventricular stimulation for clinically stable patients with normal or impaired left ventricular systolic function. Pacing Clin Electrophysiol. 2007;30(2):182–187. doi: 10.1111/j.1540-8159.2007.00647.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
