

Blood kidney injury molecule-1 is a biomarker of acute and chronic kidney injury and predicts progression to ESRD in type I diabetes
- PMID: 24904085
- PMCID: PMC4178434
- DOI: 10.1681/ASN.2013070758
Blood kidney injury molecule-1 is a biomarker of acute and chronic kidney injury and predicts progression to ESRD in type I diabetes
Abstract
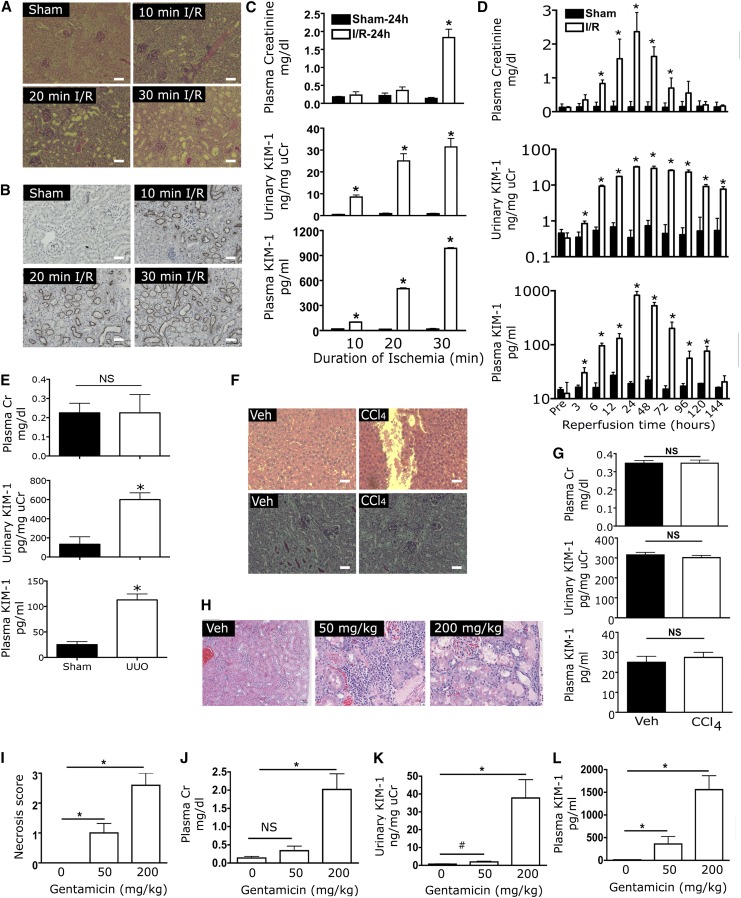
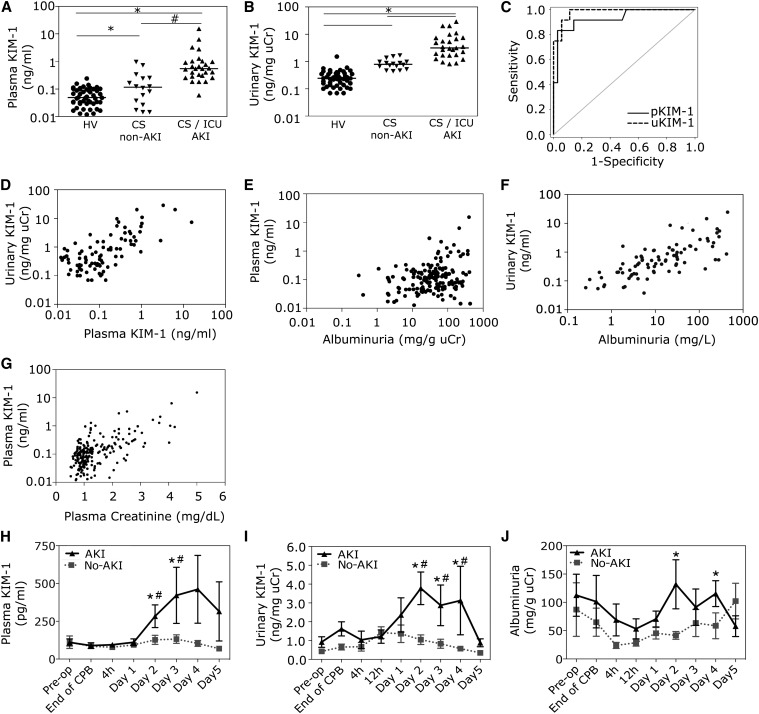
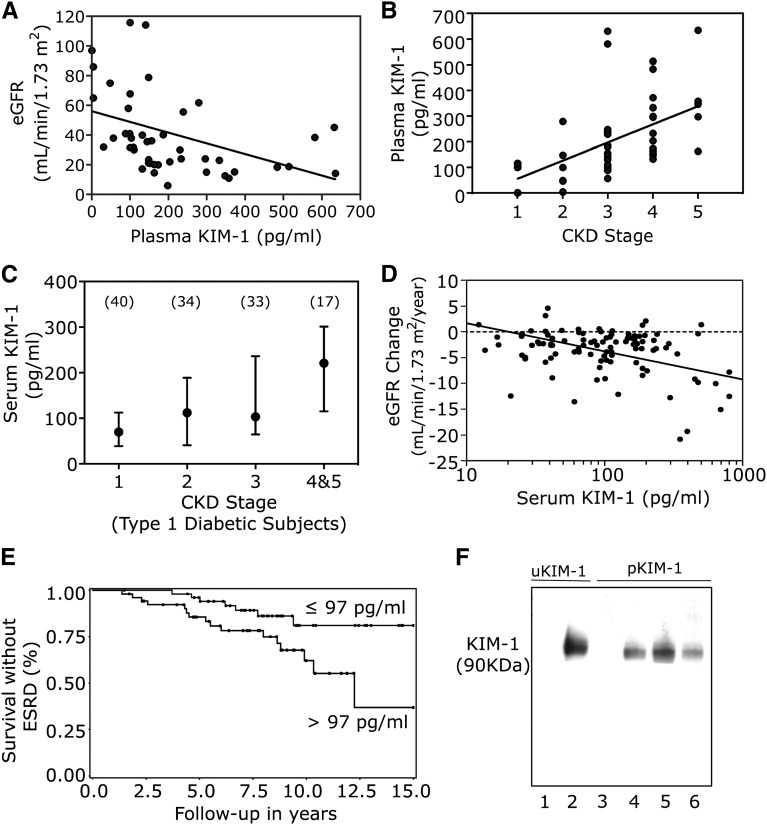
Currently, no blood biomarker that specifically indicates injury to the proximal tubule of the kidney has been identified. Kidney injury molecule-1 (KIM-1) is highly upregulated in proximal tubular cells following kidney injury. The ectodomain of KIM-1 is shed into the lumen, and serves as a urinary biomarker of kidney injury. We report that shed KIM-1 also serves as a blood biomarker of kidney injury. Sensitive assays to measure plasma and serum KIM-1 in mice, rats, and humans were developed and validated in the current study. Plasma KIM-1 levels increased with increasing periods of ischemia (10, 20, or 30 minutes) in mice, as early as 3 hours after reperfusion; after unilateral ureteral obstruction (day 7) in mice; and after gentamicin treatment (50 or 200 mg/kg for 10 days) in rats. In humans, plasma KIM-1 levels were higher in patients with AKI than in healthy controls or post-cardiac surgery patients without AKI (area under the curve, 0.96). In patients undergoing cardiopulmonary bypass, plasma KIM-1 levels increased within 2 days after surgery only in patients who developed AKI (P<0.01). Blood KIM-1 levels were also elevated in patients with CKD of varous etiologies. In a cohort of patients with type 1 diabetes and proteinuria, serum KIM-1 level at baseline strongly predicted rate of eGFR loss and risk of ESRD during 5-15 years of follow-up, after adjustment for baseline urinary albumin-to-creatinine ratio, eGFR, and Hb1Ac. These results identify KIM-1 as a blood biomarker that specifically reflects acute and chronic kidney injury.
Keywords: acute renal failure; chronic kidney disease; chronic kidney failure; nephrotoxicity.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Ichimura T, Bonventre JV, Bailly V, Wei H, Hession CA, Cate RL, Sanicola M: Kidney injury molecule-1 (KIM-1), a putative epithelial cell adhesion molecule containing a novel immunoglobulin domain, is up-regulated in renal cells after injury. J Biol Chem 273: 4135–4142, 1998 - PubMed
-
- Han WK, Bailly V, Abichandani R, Thadhani R, Bonventre JV: Kidney Injury Molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int 62: 237–244, 2002 - PubMed
-
- Ichimura T, Hung CC, Yang SA, Stevens JL, Bonventre JV: Kidney injury molecule-1: a tissue and urinary biomarker for nephrotoxicant-induced renal injury. Am J Physiol Renal Physiol 286: F552–F563, 2004 - PubMed
-
- Vaidya VS, Ozer JS, Dieterle F, Collings FB, Ramirez V, Troth S, Muniappa N, Thudium D, Gerhold D, Holder DJ, Bobadilla NA, Marrer E, Perentes E, Cordier A, Vonderscher J, Maurer G, Goering PL, Sistare FD, Bonventre JV: Kidney injury molecule-1 outperforms traditional biomarkers of kidney injury in preclinical biomarker qualification studies. Nat Biotechnol 28: 478–485, 2010 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- DK075941/DK/NIDDK NIH HHS/United States
- K23 DK075941/DK/NIDDK NIH HHS/United States
- U01-DK85660/DK/NIDDK NIH HHS/United States
- U01 DK085660/DK/NIDDK NIH HHS/United States
- MR/L006758/1/MRC_/Medical Research Council/United Kingdom
- R37 DK039773/DK/NIDDK NIH HHS/United States
- DK041526/DK/NIDDK NIH HHS/United States
- RC2 GM093080/GM/NIGMS NIH HHS/United States
- G0700654/MRC_/Medical Research Council/United Kingdom
- R01 DK041526/DK/NIDDK NIH HHS/United States
- R01 DK039773/DK/NIDDK NIH HHS/United States
- DK072381/DK/NIDDK NIH HHS/United States
- R01 DK093574/DK/NIDDK NIH HHS/United States
- R01 DK072381/DK/NIDDK NIH HHS/United States
- DK39773/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
