

Streptococcus pneumoniae carriage prevalence in Nepal: evaluation of a method for delayed transport of samples from remote regions and implications for vaccine implementation
- PMID: 24905574
- PMCID: PMC4048273
- DOI: 10.1371/journal.pone.0098739
Streptococcus pneumoniae carriage prevalence in Nepal: evaluation of a method for delayed transport of samples from remote regions and implications for vaccine implementation
Abstract
Background: Pneumococcal disease is a significant cause of morbidity and mortality in young children in Nepal, and currently available pneumococcal conjugate vaccines offer moderate coverage of invasive disease isolates.
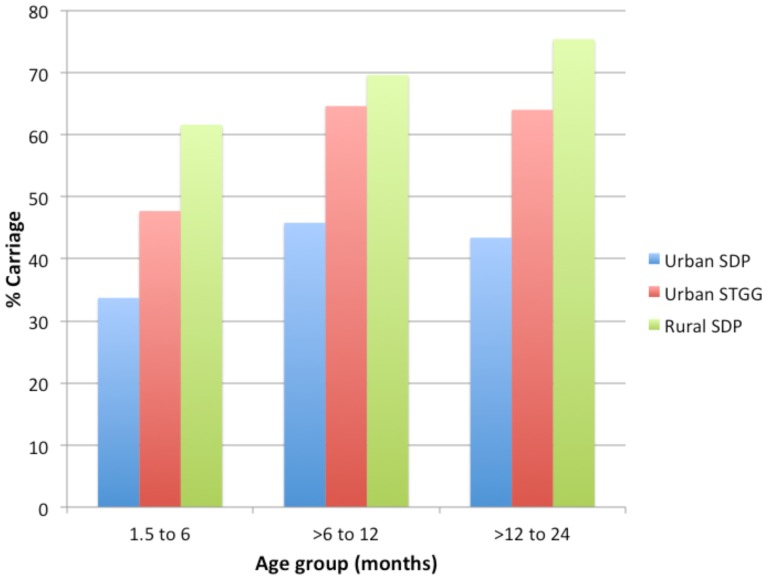
Methods: A prevalence study of children aged 1.5 to 24 months in urban and rural Nepal was conducted. In the urban group, nasopharyngeal swabs (NPS) were transported using silica desiccant packages (SDP) with delayed processing (2 weeks), or skim-milk-tryptone-glucose-glycerin (STGG) with immediate processing (within 8 hours). Pneumococcal nasopharyngeal carriage prevalence, serogroup/type distribution and isolate genotypes (as defined by multilocus sequence typing) were determined.
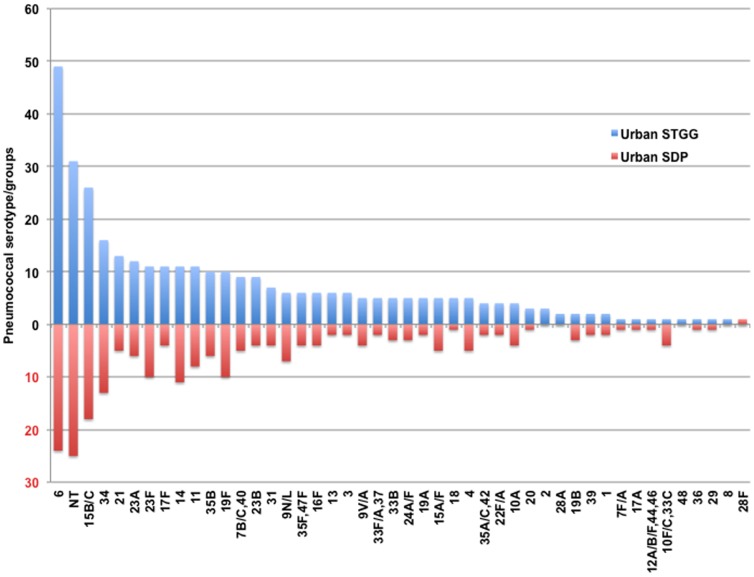
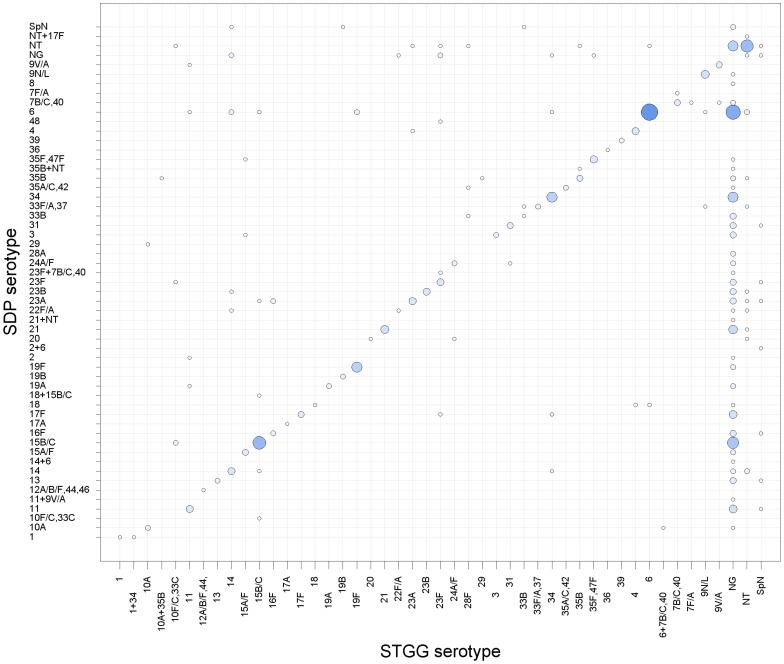
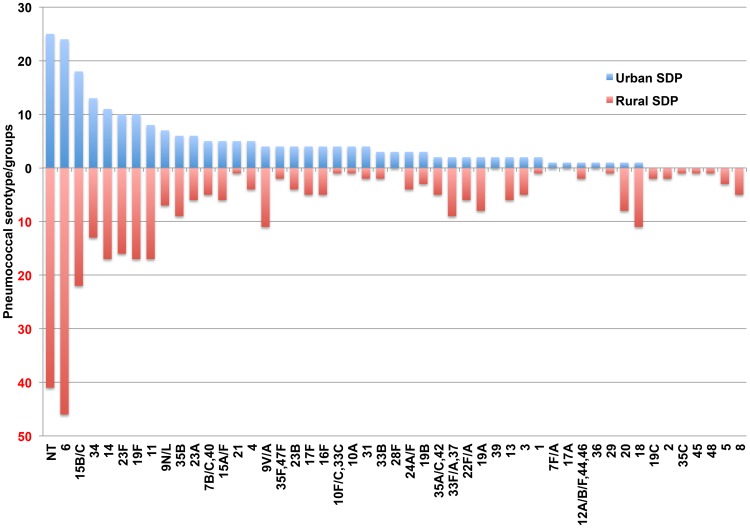
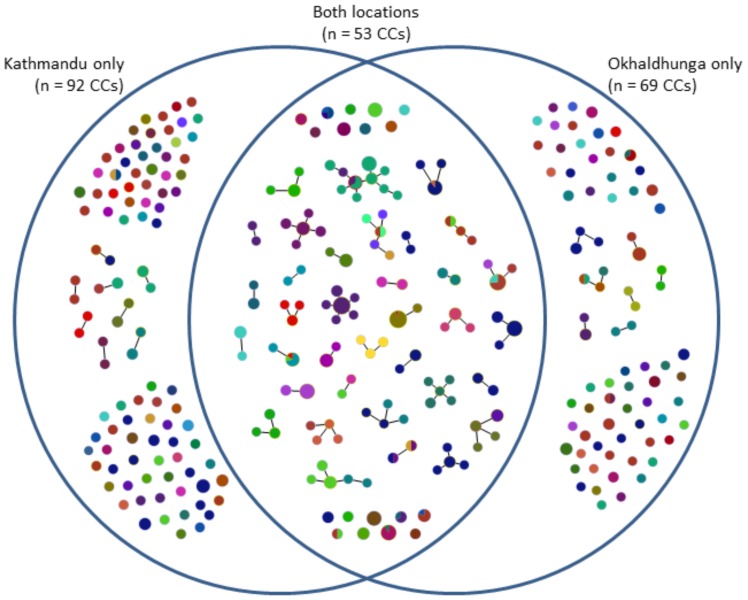
Results: 1101 children were enrolled into the study: 574 in the urban group and 527 in the rural group. Overall carriage prevalence based on culture from specimens transported and stored in STGG was 58.7% (337/574), compared to 40.9% (235/574) in SDP. There was concordance of detection of pneumococcus in 67% of samples. Using the SDP method, pneumococcal carriage prevalence was higher in the rural population (69.2%; 364/526) compared to the urban population (40.9%; 235/574). Serogroup/type distribution varied with geographical location. Over half of the genotypes identified in both the urban and rural pneumococcal populations were novel.
Conclusion: The combination of delayed culture and transport using SDP underestimates the prevalence of pneumococcal carriage; however, in remote areas, this method could still provide a useful estimate of carriage prevalence and serogroup/type distribution. Vaccine impact is unpredictable in a setting with novel genotypes and limited serotype coverage as described here. Consequently, continued surveillance of pneumococcal isolates from carriage and disease in Nepali children following the planned introduction of pneumococcal conjugate vaccines introduction will be essential.
Conflict of interest statement
Figures
References
-
- O'Brien KL, Wolfson LJ, Watt JP, Henkle E, Deloria-Knoll M, et al. (2009) Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet 374: 893–902. - PubMed
-
- Williams EJ, Thorson S, Maskey M, Mahat S, Hamaluba M, et al. (2009) Hospital-based surveillance of invasive pneumococcal disease among young children in urban Nepal. Clin Infect Dis 48 Suppl 2S114–122. - PubMed
-
- Kelly DF, Thorson S, Maskey M, Mahat S, Shrestha U, et al. (2011) The burden of vaccine-preventable invasive bacterial infections and pneumonia in children admitted to hospital in urban Nepal. Int J Infect Dis 15: e17–23. - PubMed
-
- Shah AS, Knoll MD, Sharma PR, Moisi JC, Kulkarni P, et al. (2009) Invasive pneumococcal disease in Kanti Children's Hospital, Nepal, as observed by the South Asian Pneumococcal Alliance network. Clin Infect Dis 48 Suppl 2S123–128. - PubMed
-
- Pilishvili T, Lexau C, Farley MM, Hadler J, Harrison LH, et al. (2010) Sustained reductions in invasive pneumococcal disease in the era of conjugate vaccine. J Infect Dis 201: 32–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
