

A 24-month open-label study of canakinumab in neonatal-onset multisystem inflammatory disease
- PMID: 24906637
- PMCID: PMC4258169
- DOI: 10.1136/annrheumdis-2013-204877
A 24-month open-label study of canakinumab in neonatal-onset multisystem inflammatory disease
Abstract
Objective: To study efficacy and safety of escalating doses of canakinumab, a fully human anti-IL-1β monoclonal antibody in the severe cryopyrin-associated periodic syndrome, neonatal-onset multisystem inflammatory disease (NOMID).
Methods: 6 patients were enrolled in this 24-month, open-label phase I/II study. All underwent anakinra withdrawal. The initial subcutaneous canakinumab dose was 150 mg (or 2 mg/kg in patients ≤40 kg) or 300 mg (or 4 mg/kg) with escalation up to 600 mg (or 8 mg/kg) every 4 weeks. Full remission was remission of patient-reported clinical components and measures of systemic inflammation and CNS inflammation. Hearing, vision and safety were assessed. Primary endpoint was full remission at month 6.
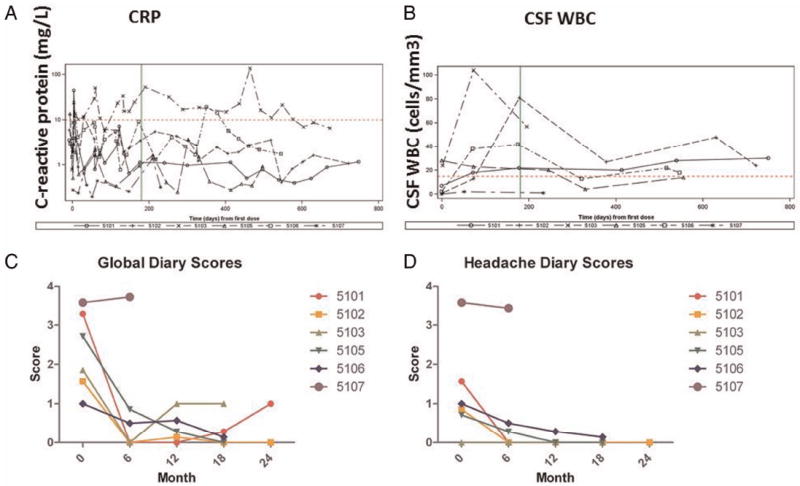
Results: All patients flared after anakinra withdrawal, and symptoms and serum inflammatory markers improved with canakinumab. All patients required dose escalation to the maximum dose. At month 6, none had full remission, although 4/6 achieved inflammatory remission, based on disease activity diary scores and normal C-reactive proteins. None had CNS remission; 5/6 due to persistent CNS leucocytosis. At the last study visit, 5/6 patients achieved inflammatory remission and 4/6 had continued CNS leucocytosis. Visual acuity and field were stable in all patients, progressive hearing loss occurred in 1/10 ears. Adverse events (AEs) were rare. One serious AE (abscess due to a methicillin-resistant Staphylococcus aureus infection) occurred.
Conclusions: Canakinumab at the studied doses improves symptoms and serum inflammatory features of NOMID, although low-grade CNS leukocytosis in four patients and headaches in one additional patient persisted. Whether further dose intensifications are beneficial in these cases remains to be assessed.
Clinicaltrialsgov identifier: NCT00770601.
Keywords: Cytokines; DMARDs (Biologic); Disease Activity; Inflammation.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
