

Impact of community based, specialist palliative care teams on hospitalisations and emergency department visits late in life and hospital deaths: a pooled analysis
- PMID: 24906901
- PMCID: PMC4048125
- DOI: 10.1136/bmj.g3496
Impact of community based, specialist palliative care teams on hospitalisations and emergency department visits late in life and hospital deaths: a pooled analysis
Abstract
Objective: To determine the pooled effect of exposure to one of 11 specialist palliative care teams providing services in patients' homes.
Design: Pooled analysis of a retrospective cohort study.
Setting: Ontario, Canada.
Participants: 3109 patients who received care from specialist palliative care teams in 2009-11 (exposed) matched by propensity score to 3109 patients who received usual care (unexposed).
Intervention: The palliative care teams studied served different geographies and varied in team composition and size but had the same core team members and role: a core group of palliative care physicians, nurses, and family physicians who provide integrated palliative care to patients in their homes. The teams' role was to manage symptoms, provide education and care, coordinate services, and be available without interruption regardless of time or day.
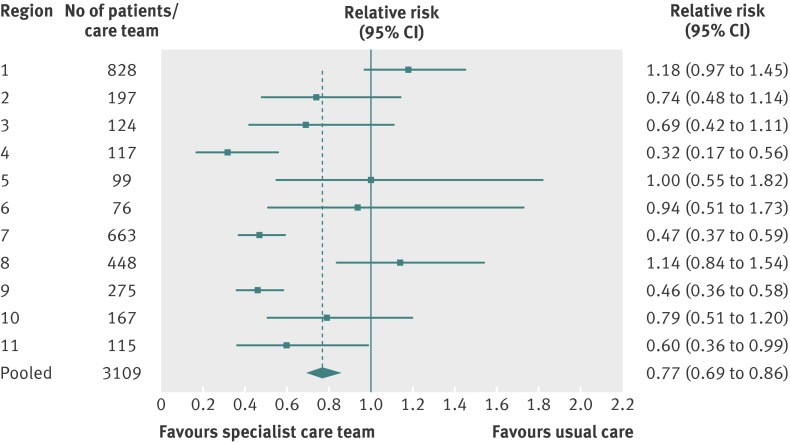
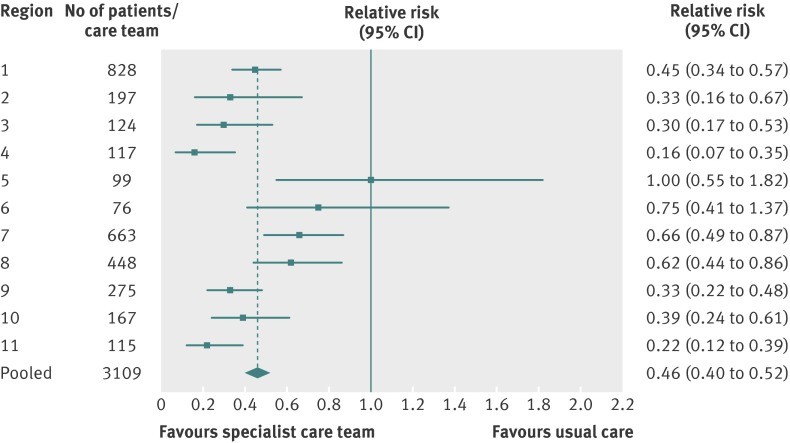
Main outcome measures: Patients (a) being in hospital in the last two weeks of life; (b) having an emergency department visit in the last two weeks of life; or (c) dying in hospital.
Results: In both exposed and unexposed groups, about 80% had cancer and 78% received end of life homecare services for the same average duration. Across all palliative care teams, 970 (31.2%) of the exposed group were in hospital and 896 (28.9%) had an emergency department visit in the last two weeks of life respectively, compared with 1219 (39.3%) and 1070 (34.5%) of the unexposed group (P<0.001). The pooled relative risks of being in hospital and having an emergency department visit in late life comparing exposed versus unexposed were 0.68 (95% confidence interval 0.61 to 0.76) and 0.77 (0.69 to 0.86) respectively. Fewer exposed than unexposed patients died in hospital (503 (16.2%) v 887 (28.6%), P<0.001), and the pooled relative risk of dying in hospital was 0.46 (0.40 to 0.52).
Conclusions: Community based specialist palliative care teams, despite variation in team composition and geographies, were effective at reducing acute care use and hospital deaths at the end of life.
© Seow et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

Comment in
-
Can palliative care teams relieve some of the pressure on acute services?BMJ. 2014 Jun 6;348:g3693. doi: 10.1136/bmj.g3693. BMJ. 2014. PMID: 24906714 No abstract available.
References
-
- Covinsky KE, Fortinsky RH, Palmer RM, Kresevic DM, Landefeld CS. Relation between symptoms of depression and health status outcomes in acutely ill hospitalized older persons. Ann Intern Med 1997;126:417-25. - PubMed
-
- Fassbender K, Fainsinger RL, Carson M, Finegan BA. Cost trajectories at the end of life: the Canadian experience. J Pain Symptom Manage 2009;38:75-80. - PubMed
-
- Higginson IJ, Sen-Gupta GJ. Place of care in advanced cancer: a qualitative systematic literature review of patient preferences. J Palliat Med 2000;3:287-300. - PubMed
-
- Paz-Ruiz S, Gomez-Batiste X, Espinosa J, Porta-Sales J, Esperalba J. The costs and savings of a regional public palliative care program: the Catalan experience at 18 years. J Pain Symptom Manage 2009;38:87-96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical