

Risk factors for obstetric morbidity in patients with uterine atony undergoing caesarean delivery
- PMID: 24907281
- PMCID: PMC4166890
- DOI: 10.1093/bja/aeu150
Risk factors for obstetric morbidity in patients with uterine atony undergoing caesarean delivery
Abstract
Background: Uterine atony (UA) is recognized as a leading cause of postpartum haemorrhage. However, knowledge of risk factors of haemorrhage-related morbidity among patients diagnosed with UA is uncertain. We investigated risk factors for haemorrhage-related morbidity among patients undergoing Caesarean delivery with UA.
Methods: We conducted a secondary analysis of data sourced from a 4-yr observational study at 19 US academic centres. Patients with UA were identified based on receiving methylergonovine or carboprost. Our primary outcome (haemorrhage-related morbidity) included a composite of intra- or postpartum transfusion; Caesarean hysterectomy; uterine or hypogastric artery ligation; intensive care admission for: pulmonary oedema, coagulopathy, adult respiratory distress syndrome, postoperative ventilation, or invasive line monitoring.
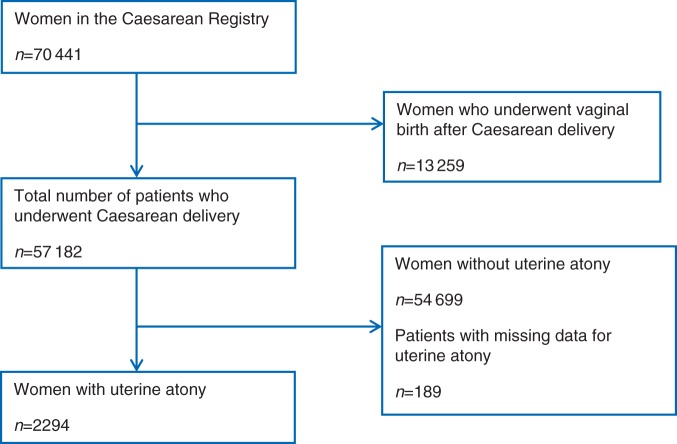
Results: Among 57,182 patients who underwent Caesarean delivery, 2294 (4%) patients developed UA. Haemorrhage-related morbidity occurred in 450 (19.6%) patients with UA. The risk of haemorrhage-related morbidity was increased among African-Americans [adjusted odds ratio (aOR)=2.36; 95% confidence interval (CI)=1.73-3.23], Hispanics (aOR=1.4; 95% CI=1.04-1.9), women with multiple gestations (aOR=1.59; 95% CI=1.06-2.38), placenta praevia (aOR=4.89; 95% CI=3.04-7.87), patients with ASA class III (aOR=1.4; 95 CI=1.03-1.9), or ASA class IV (aOR=5.88; 95% CI=2.48-13.9), exposure to general anaesthesia (GA) (aOR=2.4; 95% CI=1.59-3.62) and combined general and regional anaesthesia (aOR=4.0; 95% CI=2.62-6.09), and ≥2 prior Caesarean deliveries (aOR=1.62; 95% CI=1.1-2.39).
Conclusions: Among patients with UA undergoing Caesarean delivery, the risk of haemorrhage-related morbidity is increased in African-Americans, Hispanics, patients with multiple gestations, placenta praevia, ASA class III or IV, ≥2 prior Caesarean deliveries and those undergoing GA.
Keywords: Caesarean section; morbidity; uterine atony.
© The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
References
-
- Rossen J, Okland I, Nilsen OB, Eggebo TM. Is there an increase of postpartum hemorrhage, and is severe hemorrhage associated with more frequent use of obstetric interventions? Acta Obstet Gynecol Scand. 2010;89:1248–55. - PubMed
-
- Stones RW, Paterson CM, Saunders NJ. Risk factors for major obstetric haemorrhage. Eur J Obstet Gynecol Reprod Biol. 1993;48:15–8. - PubMed
-
- Al-Zirqi I, Vangen S, Forsen L, Stray-Pedersen B. Prevalence and risk factors of severe obstetric haemorrhage. BJOG. 2008;115:1265–72. - PubMed
-
- Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Wilson EC, Mathews TJ. Births: Final Data for 2010. Natl Vital Stat Rep. 2012;61:1. - PubMed
-
- Callaghan WM, Kuklina EV, Berg CJ. Trends in postpartum hemorrhage: United States, 1994–2006. Am J Obstet Gynecol. 2010;202:353e1–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
