

Diminished systemic and antigen-specific type 1, type 17, and other proinflammatory cytokines in diabetic and prediabetic individuals with latent Mycobacterium tuberculosis infection
- PMID: 24907382
- PMCID: PMC4215076
- DOI: 10.1093/infdis/jiu329
Diminished systemic and antigen-specific type 1, type 17, and other proinflammatory cytokines in diabetic and prediabetic individuals with latent Mycobacterium tuberculosis infection
Abstract
Background: Diabetes mellitus type 2 (DM) is known to be a major risk factor for the development of active tuberculosis, although its influence on latent Mycobacterium tuberculosis infection (hereafter, "latent infection") remains poorly characterized.
Methods: We examined circulating plasma cytokine levels in individuals with latent infection with DM or pre-DM (ie, intermediate hyperglycemia) and compared them to levels in patients with latent infection and normal glycemic control.
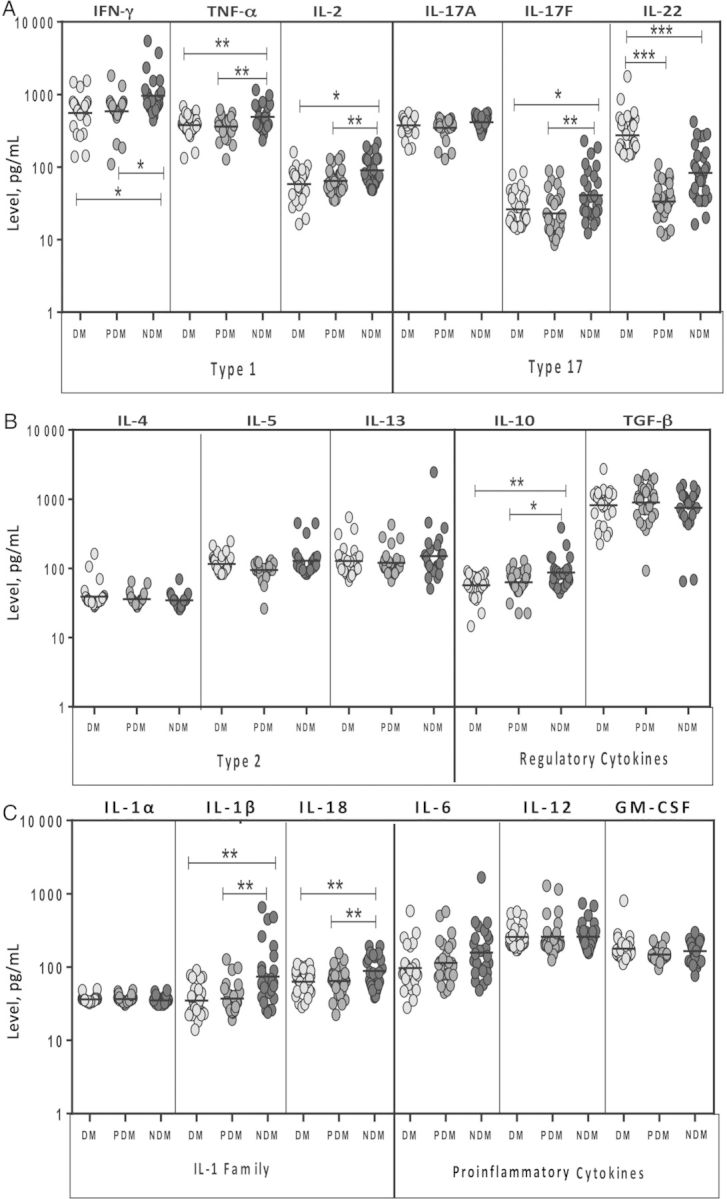
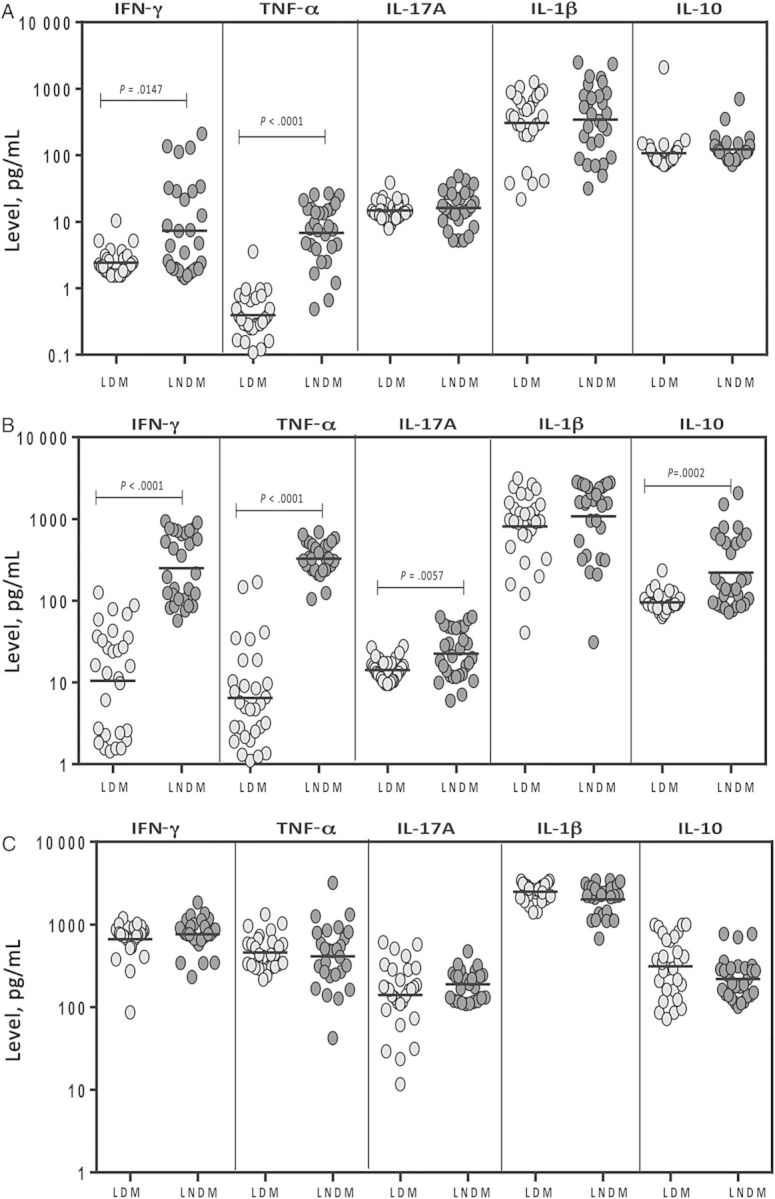
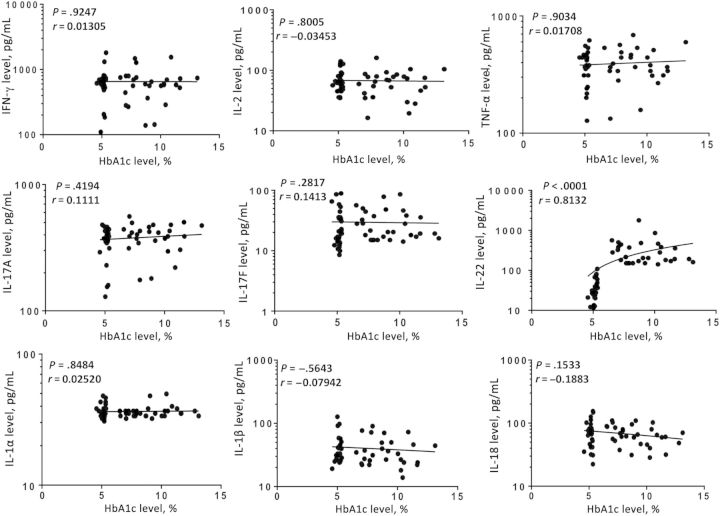
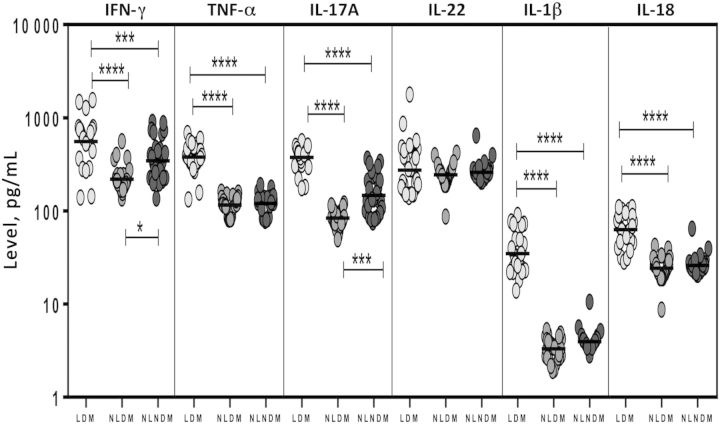
Results: In persons with DM or pre-DM, latent infection is characterized by diminished circulating levels of type 1 (interferon γ, interleukin 2, and tumor necrosis factor α) and type 17 (interleukin 17F) cytokines. This was associated with decreased systemic levels of other proinflammatory cytokines (interleukin 1β and interleukin 18) and the antiinflammatory cytokine interleukin 10 but not with decreased systemic levels of type 2 cytokines. Moreover, latently infected individuals with DM had diminished levels of spontaneous and M. tuberculosis antigen-specific levels of type 1 and type 17 cytokines when antigen-stimulated whole blood was examined. Finally, there was no significant correlation between the levels of any of the cytokines measured (with the exception of interleukin 22) with hemoglobin A1c levels.
Conclusions: Our data reveal that latent infection in the presence of DM or pre-DM, is characterized by diminished production of cytokines, implicated in the control of M. tuberculosis activation, allowing for a potential immunological mechanism that could account for the increased risk of active tuberculosis in latently infected individuals with DM.
Keywords: bacterial; cytokines; diabetes; pre-diabetes; tuberculosis.
Published by Oxford University Press on behalf of the Infectious Diseases Society of America 2014. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
