

Venovenous perfusion-induced systemic hyperthermia: five-day sheep survival studies
- PMID: 24908352
- PMCID: PMC4856431
- DOI: 10.1016/j.jtcvs.2014.04.045
Venovenous perfusion-induced systemic hyperthermia: five-day sheep survival studies
Abstract
Objective: Since hyperthermia selectively kills lung cancer cells, we developed a venovenous perfusion-induced systemic hyperthermia system for advanced lung cancer therapy. Our objective was to test the safety and accuracy of our venovenous perfusion-induced systemic hyperthermia system in 5-day sheep survival studies, following Good Laboratory Practice standards.
Methods: Our venovenous perfusion-induced systemic hyperthermia system, which included a double-lumen cannula (Avalon Elite, Rancho Dominguez, Calif), a centrifugal pump (Bio-Pump 560; Medtronic Inc, Minneapolis, Minn), a heat exchanger (BIOtherm; Medtronic Perfusion Systems, Brooklyn Park, Minn), and a heater/cooler (modified Blanketrol IIIl Cincinnati Subzero, Cincinnati, Ohio), was tested in healthy adult sheep (n=5). The perfusion circuit was primed with prewarmed Plasma-Lyte A (Baxter Healthcare Corp, Deerfield, Ill) and de-aired. Calibrated temperature probes were placed in the right and left sides of the nasopharynx, bladder, and blood in/out tubing in the animal. The double-lumen cannula was inserted through the jugular vein into the superior vena cava, with the tip in the inferior vena cava.
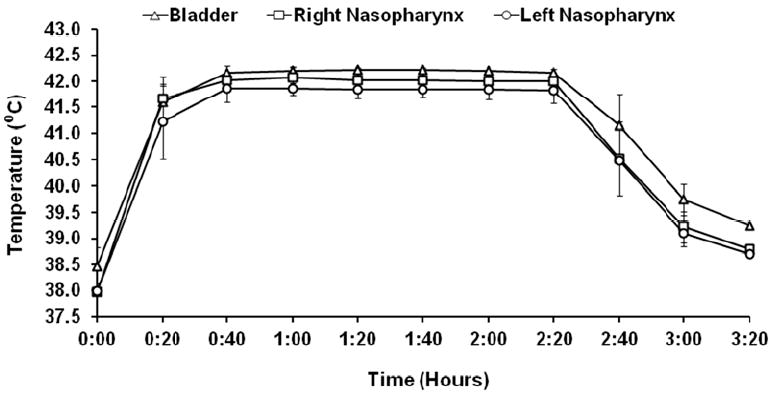
Results: Therapeutic core temperature (42°C-42.5°C), calculated from the right and left sides of the nasopharynx and bladder temperatures, was achieved in all sheep. Heating time was 21±5 minutes. Therapeutic core temperature was maintained for 120 minutes followed by a cooling phase (35±6 minutes) to reach baseline temperature. All sheep recovered from anesthesia with spontaneous breathing within 4 hours. Arterial, pulmonary, and central venous pressures were stable. Transient increases in heart rate, cardiac output, and blood glucose occurred during hyperthermia but returned to normal range after venovenous perfusion-induced systemic hyperthermia termination. Electrolytes, complete blood counts, and metabolism enzymes were within normal to near normal range throughout the study. No significant venovenous perfusion-induced systemic hyperthermia-related hemolysis was observed. Neurologic assessment showed normal brain function all 5 days.
Conclusions: Our venovenous perfusion-induced systemic hyperthermia system safely delivered the hyperthermia dose with no significant hyperthermia-related complications.
Copyright © 2014 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Stinchcombe TE, Socinski MA. Current treatments for advanced stage non-small cell lung cancer. Proc Am Thorac Soc. 2009;6:233–41. - PubMed
-
- Scagliotti GV, Krzakowski M, Szczesna A, Strausz J, Makhson A, Reck M, et al. Sunitinib plus erlotinib versus placebo plus erlotinib in patients with previously treated advanced non-small-cell lung cancer: a phase III trial. J Clin Oncol. 2012;30:2070–8. - PubMed
-
- Gridelli C, Ciardiello F, Gallo C, Feld R, Butts C, Gebbia V, et al. First-line erlotinib followed by second-line cisplatin-gemcitabine chemotherapy in advanced non-small-cell lung cancer: the TORCH randomized trial. J Clin Oncol. 2012;30:3002–11. - PubMed
-
- Lynch TJ, Bondarenko I, Luft A, Serwatowski P, Barlesi F, Chacko R, et al. Ipilimumab in combination with paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from a randomized, doubleblind, multicenter phase II study. J Clin Oncol. 2012;30:2046–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
