

Improving adherence to antiretroviral treatment in Uganda with a low-resource facility-based intervention
- PMID: 24909408
- PMCID: PMC4049133
- DOI: 10.3402/gha.v7.24198
Improving adherence to antiretroviral treatment in Uganda with a low-resource facility-based intervention
Abstract
Objective: To assess the effects of facility-based interventions using existing resources to improve overall patient attendance and adherence to antiretroviral therapy (ART) at ART-providing facilities in Uganda.
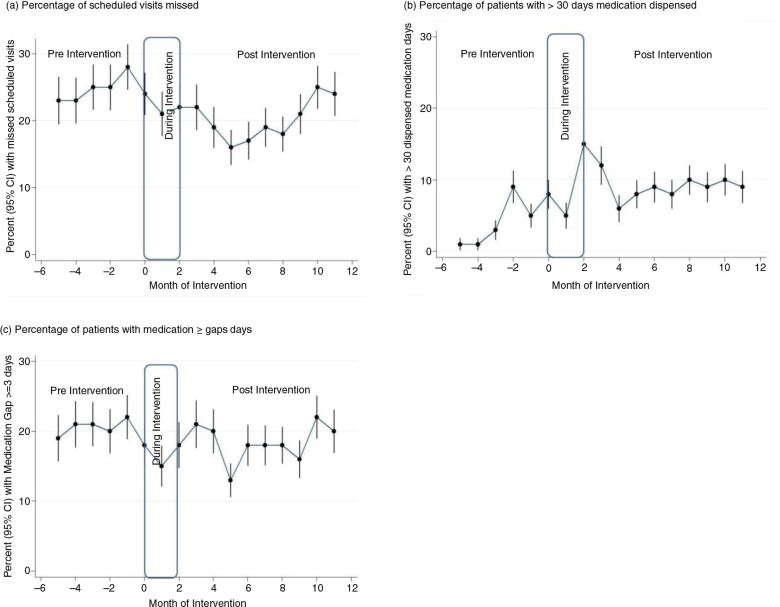
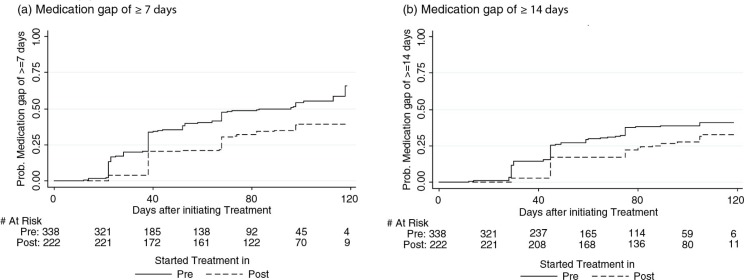
Methods: This was an interventional study which tracked attendance and treatment adherence of two distinct cohorts: experienced patients who had been on treatment for at least 12 months prior to the intervention and patients newly initiated on ART before or during the intervention. The interventions included instituting appointment system, fast-tracking, and giving longer prescriptions to experienced stable patients. Mixed-effects models were used to examine intervention effects on the experienced patients, while Cox proportional hazards models were used to determine the intervention effects on time until newly treated patients experienced gaps in medication availability.
Results: In all, 1481 patients' files were selected for follow-up from six facilities--720 into the experienced cohort, and 761 into the newly treated cohort. Among patients in the experienced cohort, the interventions were associated with a significant reduction from 24.4 to 20.3% of missed appointments (adjusted odds ratio (AOR): 0.67; 95% confidence interval (CI): 0.59-0.77); a significant decrease from 20.2 to 18.4% in the medication gaps of three or more days (AOR: 0.69; 95% CI: 0.60-0.79); and a significant increase from 4.3 to 9.3% in the proportion of patients receiving more than 30 days of dispensed medication (AOR: 2.35; 95% CI: 1.91-2.89). Among newly treated patients, the interventions were associated with significant reductions of 44% (adjusted hazard rate (AHR): 0.56, 95% CI: 0.42-0.74) and 38% (AHR: 0.62; 95% CI: 0.45-0.85) in the hazards of experiencing a medication gap of 7 and 14 days or more, respectively.
Conclusions: Patients' adherence was improved with low-cost and easily implemented interventions using existing health facilities' resources. We recommend that such interventions be considered for scale-up at national levels as measures to improve clinic attendance and ART adherence among patients in Uganda and other low-resource settings in sub-Saharan Africa.
Keywords: Uganda; adherence; antiretroviral therapy; intervention; management; staff motivation.
Figures
References
-
- Agnarson AM, Masanja H, Ekstrom AM, Eriksen J, Tomson G, Thorson A. Challenges to ART scale-up in a rural district in Tanzania: stigma and distrust among Tanzanian health care workers, people living with HIV and community members. Trop Med Int Health. 2010;15:1000–7. - PubMed
-
- Hanefeld J. The impact of Global Health Initiatives at national and sub-national level—a policy analysis of their role in implementation processes of antiretroviral treatment (ART) roll-out in Zambia and South Africa. AIDS Care. 2010;22(Suppl 1):93–102. - PubMed
-
- Uebel KE, Timmerman V, Ingle SM, van Rensburg DH, Mollentze WF. Towards universal ARV access: achievements and challenges in Free State Province, South Africa. S Afr Med J. 2010;100:589–93. - PubMed
-
- World Health Organization, UNAIDS. Geneva: WHO; 2006. Progress on global access to HIV antiretroviral therapy. A report on “3 by 5” and beyond. 2006. http://www.who.int/hiv/progreport2006_en.pdf [cited 2014 January].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous