

A novel mouse model of endometriosis mimics human phenotype and reveals insights into the inflammatory contribution of shed endometrium
- PMID: 24910298
- PMCID: PMC4076466
- DOI: 10.1016/j.ajpath.2014.03.011
A novel mouse model of endometriosis mimics human phenotype and reveals insights into the inflammatory contribution of shed endometrium
Abstract
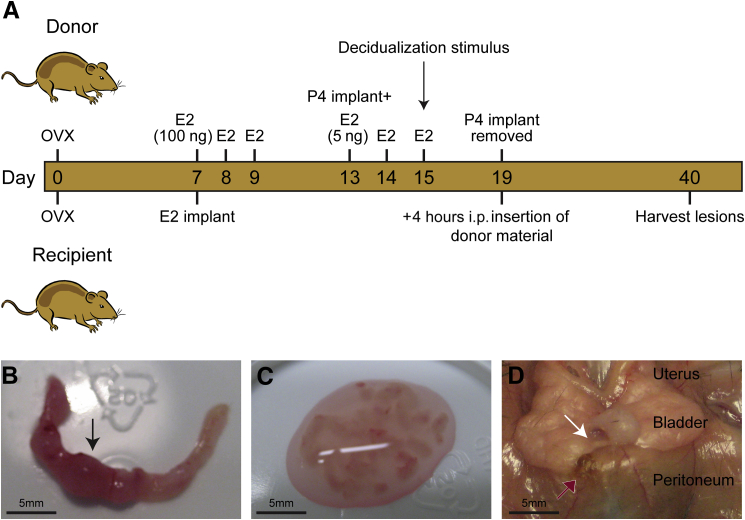
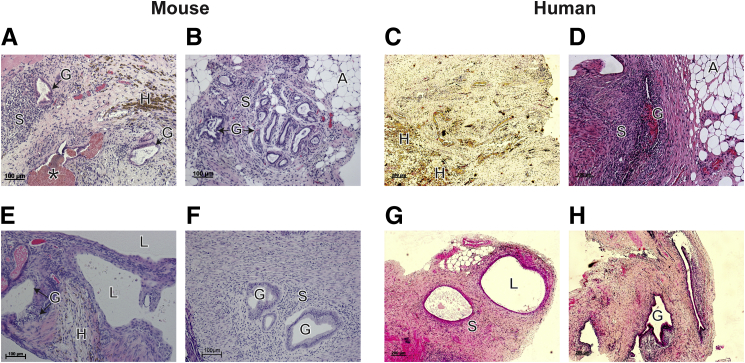
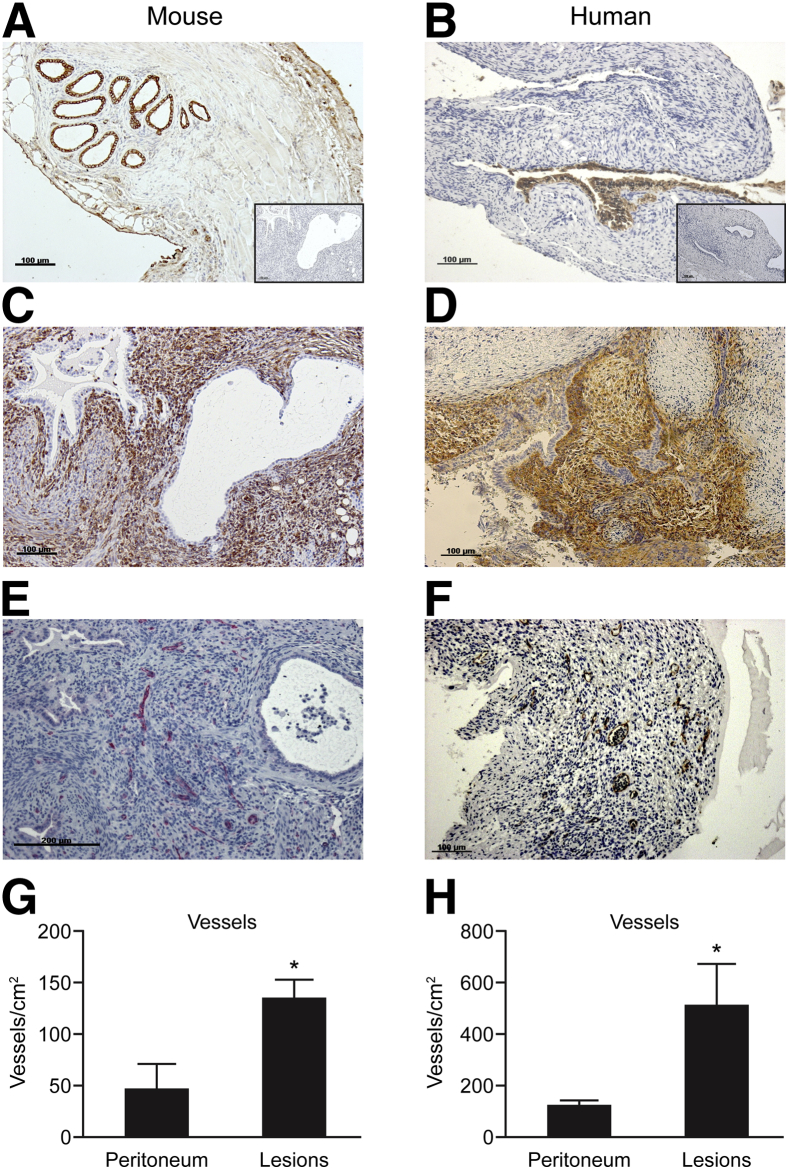
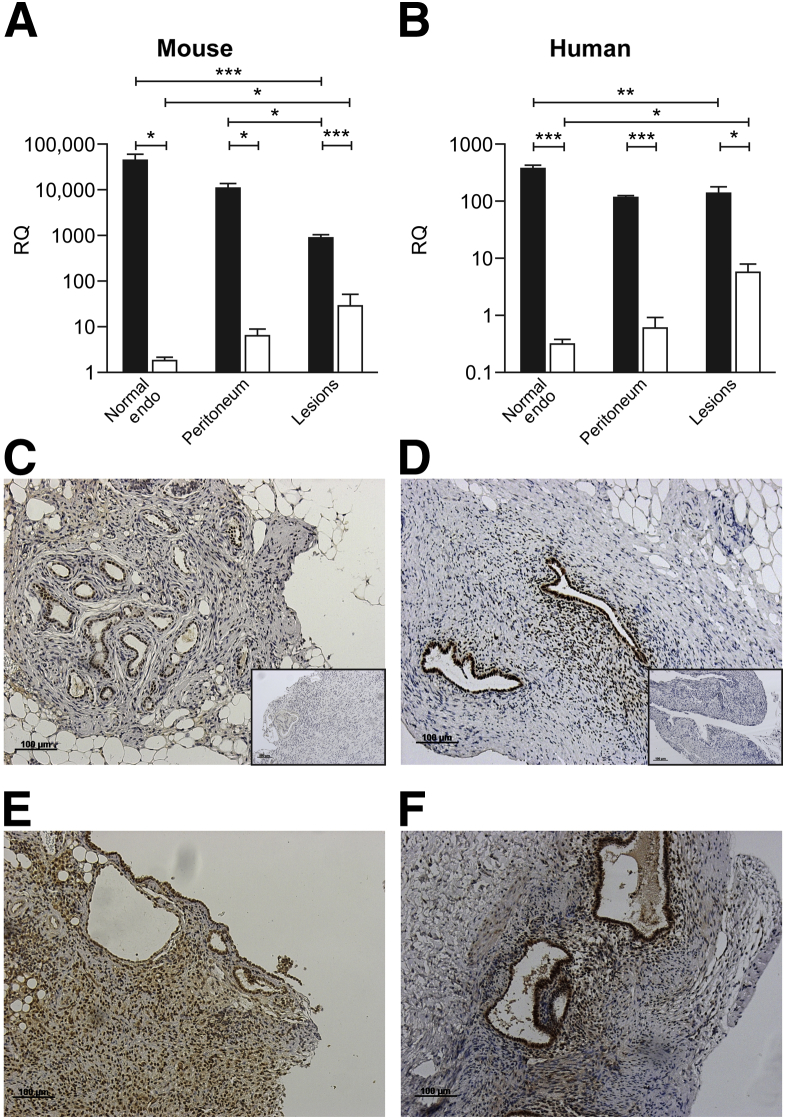
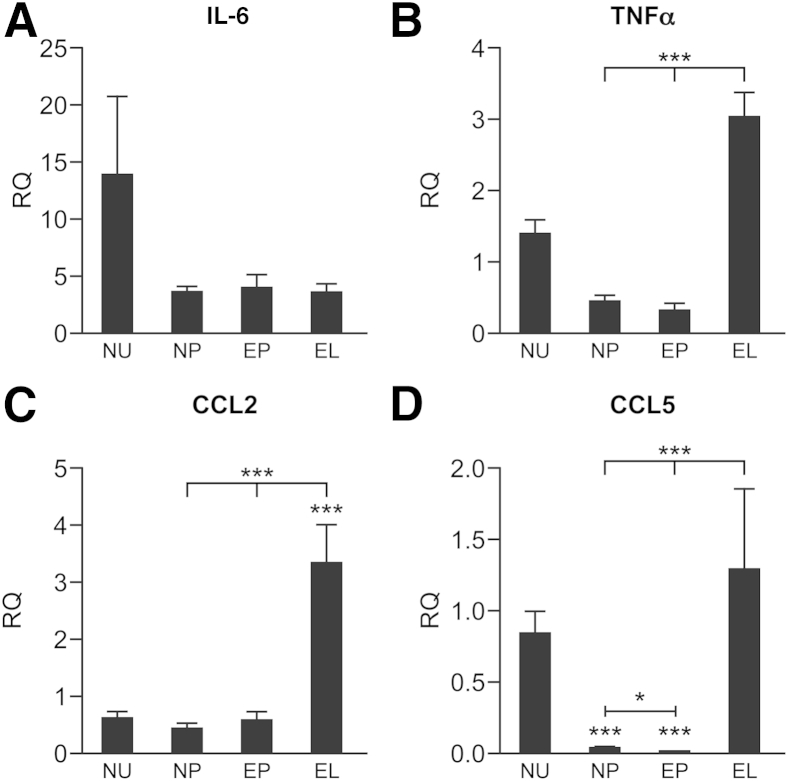
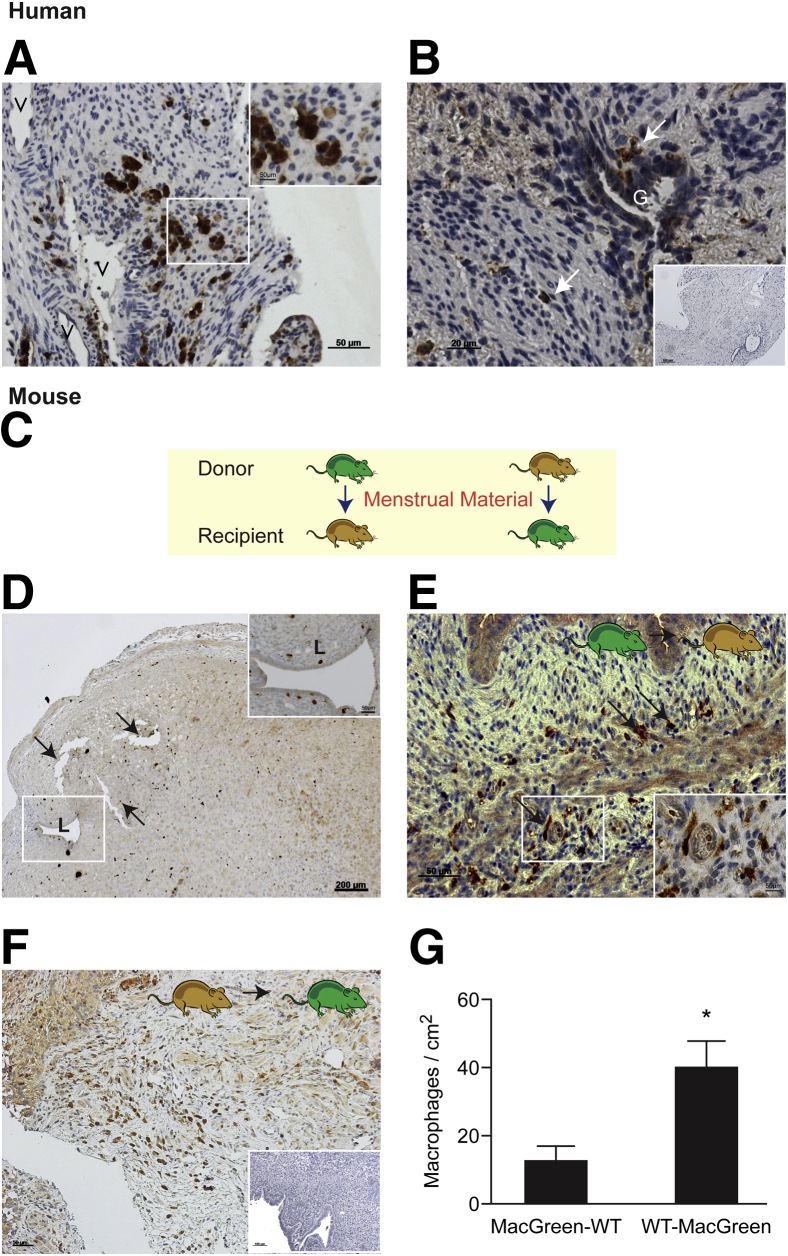
Endometriosis is an estrogen-dependent inflammatory disorder characterized by the presence of endometrial tissue outside the uterine cavity. Patients experience chronic pelvic pain and infertility, with the most likely origin of the tissue deposits (lesions) being endometrial fragments shed at menses. Menstruation is an inflammatory process associated with a dramatic increase in inflammatory mediators and tissue-resident immune cells. In the present study, we developed and validated a mouse model of endometriosis using syngeneic menstrual endometrial tissue introduced into the peritoneum of immunocompetent mice. We demonstrate the establishment of endometriotic lesions that exhibit similarities to those recovered from patients undergoing laparoscopy. Specifically, in both cases, lesions had epithelial (cytokeratin(+)) and stromal (vimentin/CD10(+)) cell compartments with a well-developed vasculature (CD31(+) endothelial cells). Expression of estrogen receptor β was increased in lesions compared with the peritoneum or eutopic endometrium. By performing experiments using mice with green fluorescent protein-labeled macrophages (MacGreen) in reciprocal transfers with wild-type mice, we obtained evidence that macrophages present in the peritoneum and in menses endometrium can contribute to the inflammatory microenvironment of the lesions. In summary, we developed a mouse model of endometriosis that exhibits similarities to human peritoneal lesions with respect to estrogen receptor expression, inflammation, and macrophage infiltration, providing an opportunity for further studies and the possible identification of novel therapies for this perplexing disorder.
Copyright © 2014 American Society for Investigative Pathology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Giudice L.C., Kao L.C. Endometriosis. Lancet. 2004;364:1789–1799. - PubMed
-
- Simoens S., Dunselman G., Dirksen C., Hummelshoj L., Bokor A., Brandes I., Brodszky V., Canis M., Colombo G.L., DeLeire T., Falcone T., Graham B., Halis G., Horne A., Kanj O., Kjer J.J., Kristensen J., Lebovic D., Mueller M., Vigano P., Wullschleger M., D'Hooghe T. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod. 2012;27:1292–1299. - PubMed
-
- Young V.J., Brown J.K., Saunders P.T., Horne A.W. The role of the peritoneum in the pathogenesis of endometriosis. Hum Reprod Update. 2013;19:558–569. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
