

Effect of tonic pain on motor acquisition and retention while learning to reach in a force field
- PMID: 24911814
- PMCID: PMC4049621
- DOI: 10.1371/journal.pone.0099159
Effect of tonic pain on motor acquisition and retention while learning to reach in a force field
Abstract
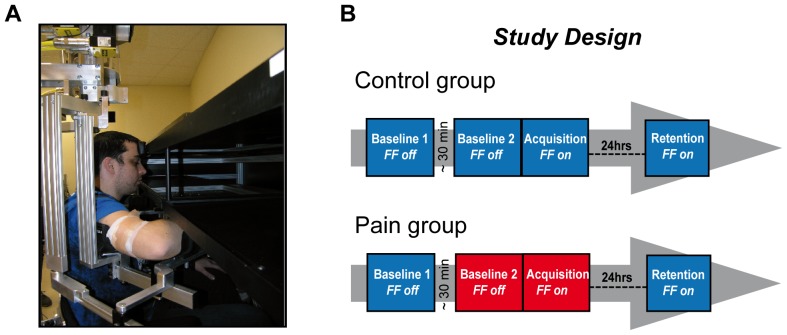
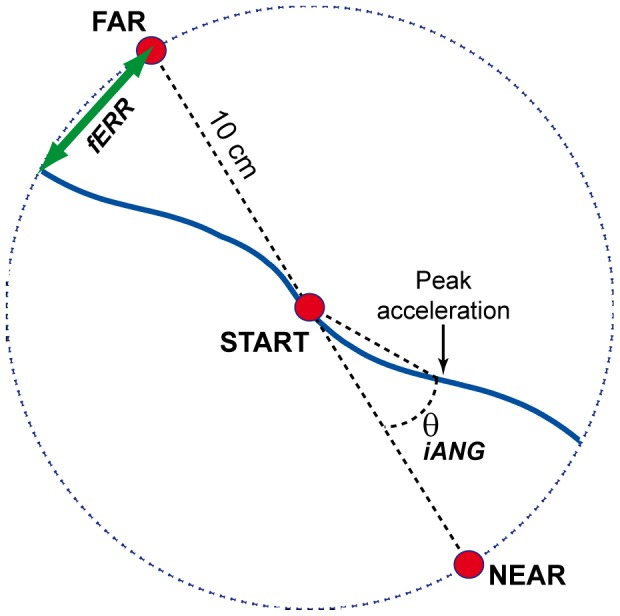
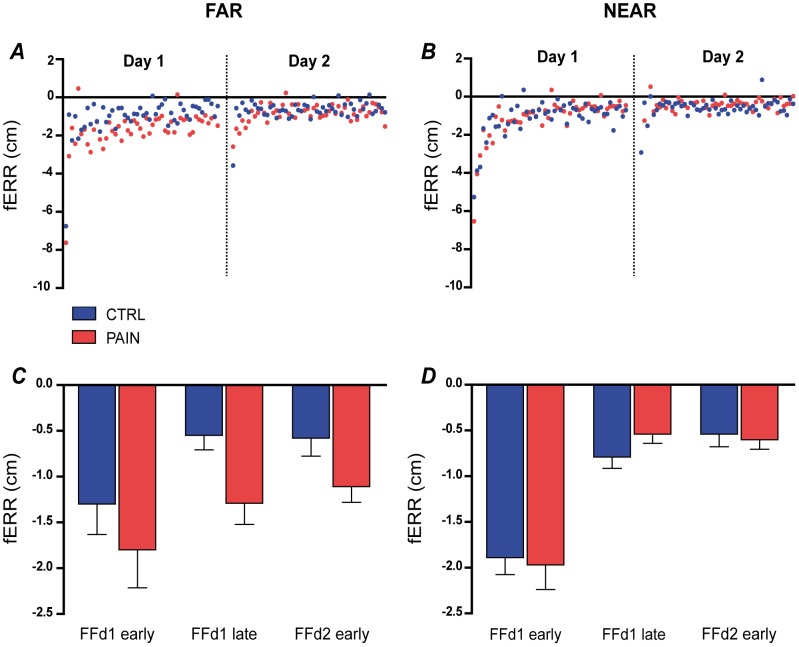
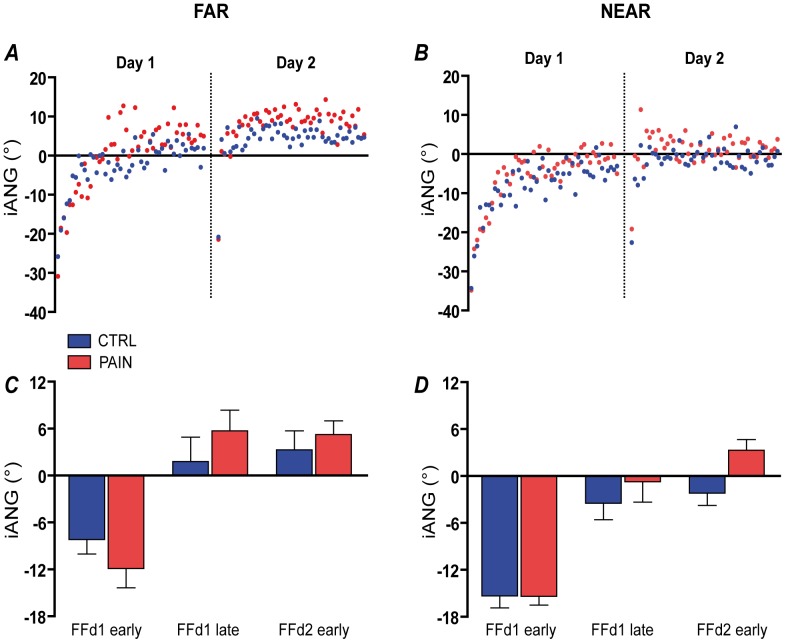
Most patients receiving intensive rehabilitation to improve their upper limb function experience pain. Despite this, the impact of pain on the ability to learn a specific motor task is still unknown. The aim of this study was to determine whether the presence of experimental tonic pain interferes with the acquisition and retention stages of motor learning associated with training in a reaching task. Twenty-nine healthy subjects were randomized to either a Control or Pain Group (receiving topical capsaicin cream on the upper arm during training on Day 1). On two consecutive days, subjects made ballistic movements towards two targets (NEAR/FAR) using a robotized exoskeleton. On Day 1, the task was performed without (baseline) and with a force field (adaptation). The adaptation task was repeated on Day 2. Task performance was assessed using index distance from the target at the end of the reaching movement. Motor planning was assessed using initial angle of deviation of index trajectory from a straight line to the target. Results show that tonic pain did not affect baseline reaching. Both groups improved task performance across time (p<0.001), but the Pain group showed a larger final error (under-compensation) than the Control group for the FAR target (p = 0.030) during both acquisition and retention. Moreover, a Group x Time interaction (p = 0.028) was observed on initial angle of deviation, suggesting that subjects with Pain made larger adjustments in the feedforward component of the movement over time. Interestingly, behaviour of the Pain group was very stable from the end of Day 1 (with pain) to the beginning of Day 2 (pain-free), indicating that the differences observed could not solely be explained by the impact of pain on immediate performance. This suggests that if people learn to move differently in the presence of pain, they might maintain this altered strategy over time.
Conflict of interest statement
Figures
References
-
- Lundstrom E, Smits A, Terent A, Borg J (2009) Risk factors for stroke-related pain 1 year after first-ever stroke. Eur J Neurol 16: 188–193. - PubMed
-
- Roosink M, Renzenbrink GJ, Buitenweg JR, Van Dongen RT, Geurts AC, et al. (2011) Persistent shoulder pain in the first 6 months after stroke: results of a prospective cohort study. Arch Phys Med Rehabil 92: 1139–1145. - PubMed
-
- Jensen TS, Krebs B, Nielsen J, Rasmussen P (1985) Immediate and long-term phantom limb pain in amputees: incidence, clinical characteristics and relationship to pre-amputation limb pain. Pain 21: 267–278. - PubMed
-
- Kooijman CM, Dijkstra PU, Geertzen JH, Elzinga A, van der Schans CP (2000) Phantom pain and phantom sensations in upper limb amputees: an epidemiological study. Pain 87: 33–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
