

A flexible simulation platform to quantify and manage emergency department crowding
- PMID: 24912662
- PMCID: PMC4059027
- DOI: 10.1186/1472-6947-14-50
A flexible simulation platform to quantify and manage emergency department crowding
Abstract
Background: Hospital-based Emergency Departments are struggling to provide timely care to a steadily increasing number of unscheduled ED visits. Dwindling compensation and rising ED closures dictate that meeting this challenge demands greater operational efficiency.
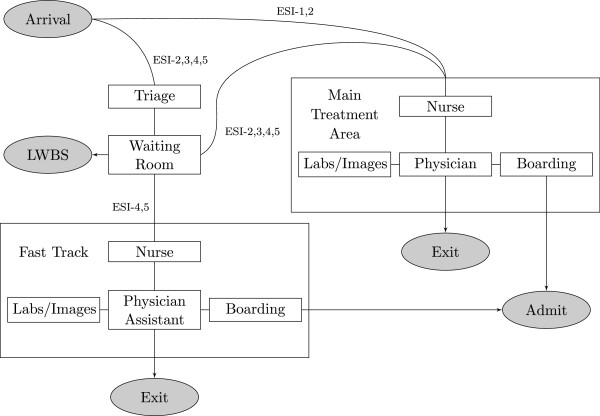
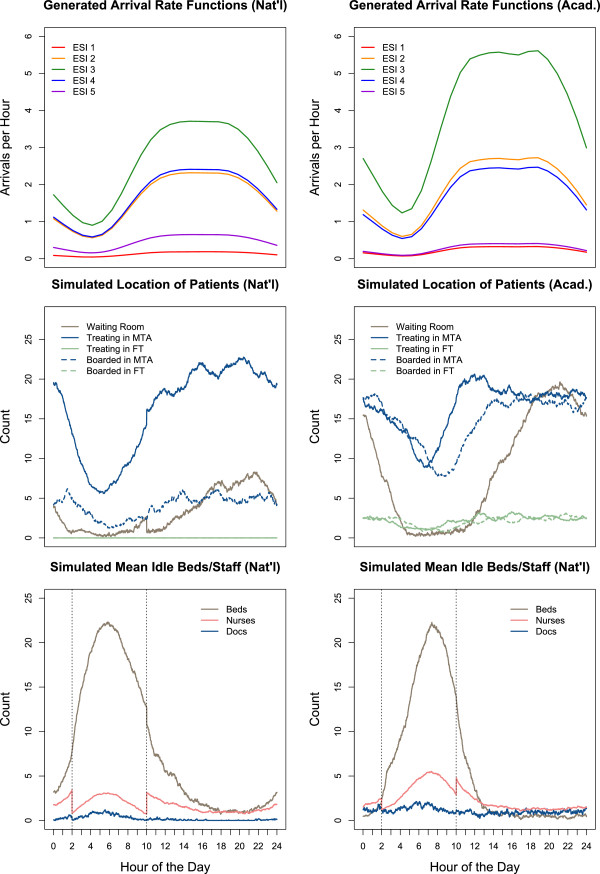
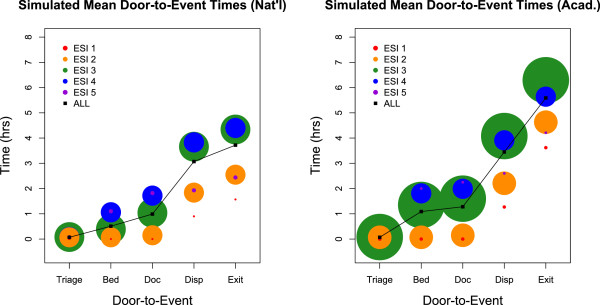
Methods: Using techniques from operations research theory, as well as a novel event-driven algorithm for processing priority queues, we developed a flexible simulation platform for hospital-based EDs. We tuned the parameters of the system to mimic U.S. nationally average and average academic hospital-based ED performance metrics and are able to assess a variety of patient flow outcomes including patient door-to-event times, propensity to leave without being seen, ED occupancy level, and dynamic staffing and resource use.
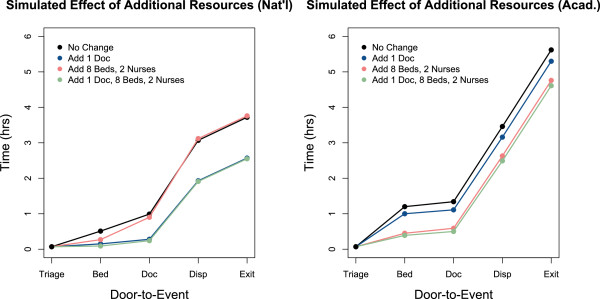
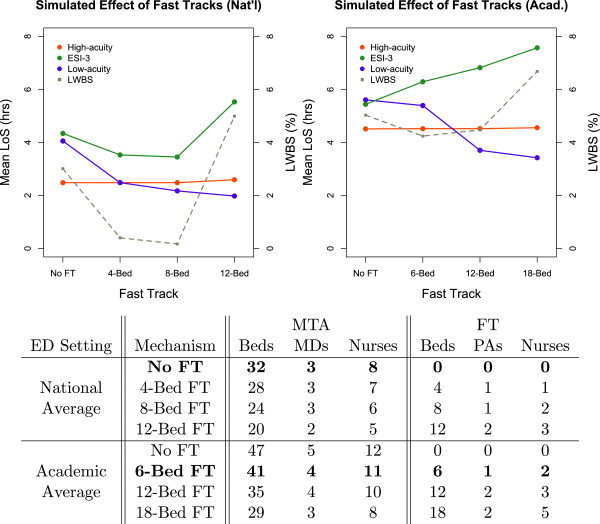
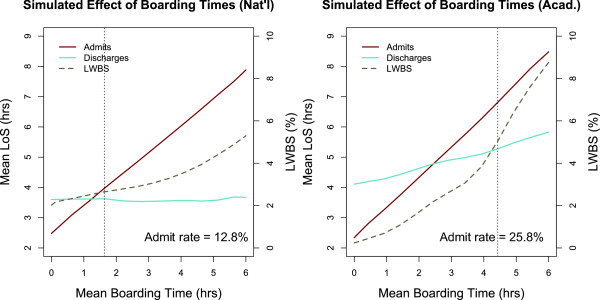
Results: The causes of ED crowding are variable and require site-specific solutions. For example, in a nationally average ED environment, provider availability is a surprising, but persistent bottleneck in patient flow. As a result, resources expended in reducing boarding times may not have the expected impact on patient throughput. On the other hand, reallocating resources into alternate care pathways can dramatically expedite care for lower acuity patients without delaying care for higher acuity patients. In an average academic ED environment, bed availability is the primary bottleneck in patient flow. Consequently, adjustments to provider scheduling have a limited effect on the timeliness of care delivery, while shorter boarding times significantly reduce crowding. An online version of the simulation platform is available at http://spark.rstudio.com/klopiano/EDsimulation/.
Conclusion: In building this robust simulation framework, we have created a novel decision-support tool that ED and hospital managers can use to quantify the impact of proposed changes to patient flow prior to implementation.
Figures
References
-
- Pitts SR, Pines JM, Handrigan MT, Kellermann AL. National trends in emergency department occupancy, 2001 to 2008, effect of inpatient admissions versus emergency department practice intensity . Ann Emerg Med. 2012;60(6):679–6863. doi: 10.1016/j.annemergmed.2012.05.014. doi:10.1016/j.annemergmed.2012.05.014. - DOI - PubMed
-
- Morganti KG, Bauhoff S, Blanchard J, Abir M, Iyer N, Smith A, Vesely JV, Okeke EN, Kellermann AL. The evolving role of emergency departments in the United States . Technical report, Rand Corporation. 2013, [ http://www.rand.org/pubs/research\_reports/RR280/] - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
