

Application of a physiologically based pharmacokinetic model informed by a top-down approach for the prediction of pharmacokinetics in chronic kidney disease patients
- PMID: 24912798
- PMCID: PMC4147047
- DOI: 10.1208/s12248-014-9626-3
Application of a physiologically based pharmacokinetic model informed by a top-down approach for the prediction of pharmacokinetics in chronic kidney disease patients
Abstract
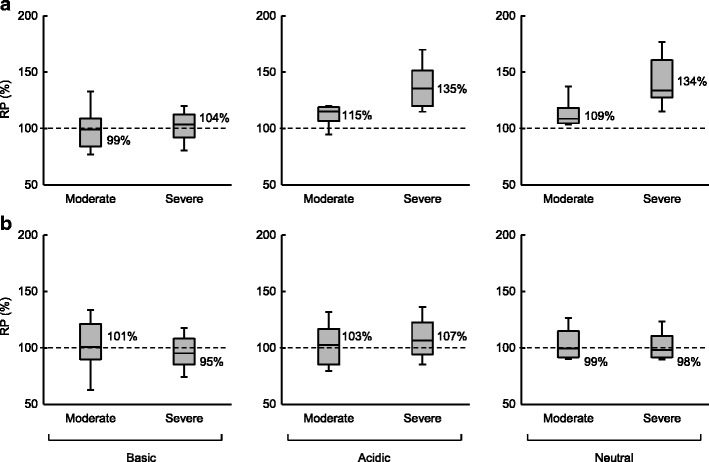
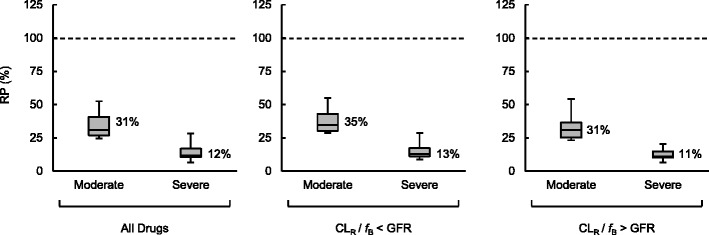
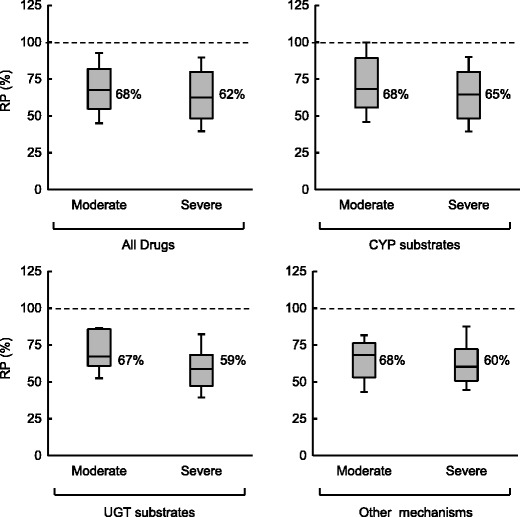
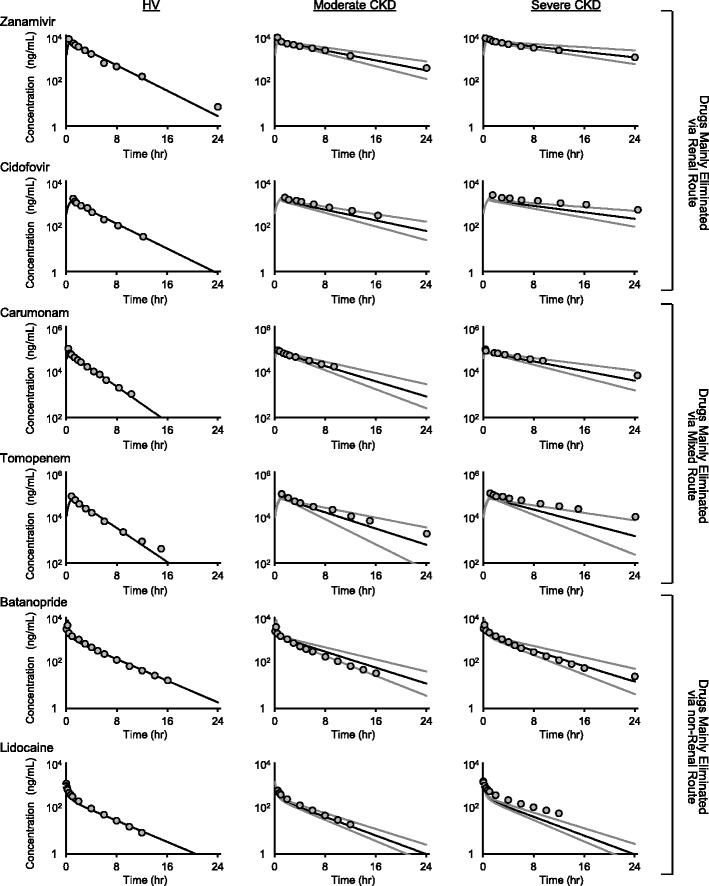
Quantitative prediction of the impact of chronic kidney disease (CKD) on drug disposition has become important for the optimal design of clinical studies in patients. In this study, clinical data of 151 compounds under CKD conditions were extensively surveyed, and alterations in pharmacokinetic parameters were evaluated. In CKD patients, the unbound hepatic intrinsic clearance decreased to a similar extent for drugs eliminated via hepatic metabolism by cytochrome P450, UDP-glucuronosyltransferase, and other mechanisms. Renal clearance showed a similar decrease to glomerular filtration rate, irrespective of the contribution of tubular secretion. The scaling factor (SF) obtained from the interquartile range of the relative change in each parameter was applied to the well-stirred model to predict clearance in patients. Hepatic and renal clearance could be successfully predicted for approximately half and two-thirds, respectively, of the applied compounds, showing the high utility of SFs. SFs were also introduced to a physiologically based pharmacokinetic (PBPK) model, and the plasma concentration profiles of 12 model compounds with different elimination pathways were predicted for CKD patients. The PBPK model combined with SFs provided good predictability for plasma concentration. The developed PBPK model with information on SFs would accelerate translational research in drug development by predicting pharmacokinetics in CKD patients.
Figures
References
-
- 2013 USRDS annual data report. Available from: www.usrds.org/adr.aspx.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
