

Demographics, clinical characteristics, health resource utilization and cost of chronic thromboembolic pulmonary hypertension patients: retrospective results from six European countries
- PMID: 24912804
- PMCID: PMC4069093
- DOI: 10.1186/1472-6963-14-246
Demographics, clinical characteristics, health resource utilization and cost of chronic thromboembolic pulmonary hypertension patients: retrospective results from six European countries
Abstract
Background: Chronic Thromboembolic Pulmonary Hypertension (CTEPH) results from incomplete resolution of a pulmonary embolus, leading to pulmonary hypertension and progressive right heart failure and death. We aimed to describe the demographics, treatment patterns, health resource utilization and related costs of patients with CTEPH.
Methods: In specialized PH centres across six European countries, medical charts of CTEPH patients on PH medication were retrospectively extracted (chart review between 2006 and 2009). Resource utilization was valued using country-specific unit costs. Descriptive statistical analyses were performed.
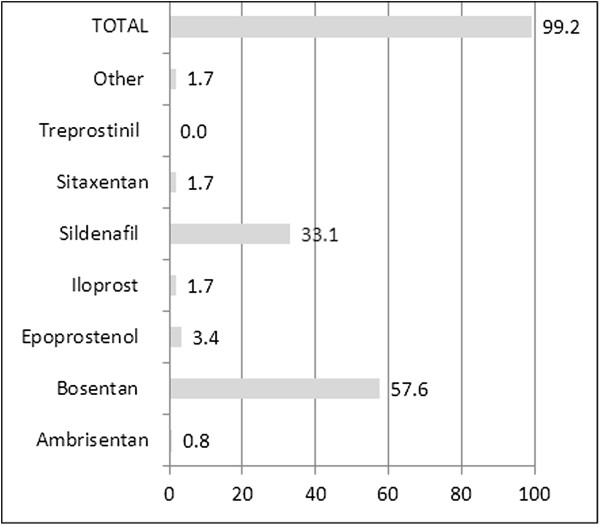
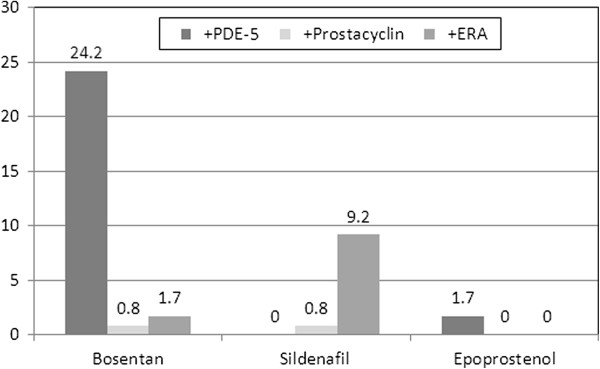
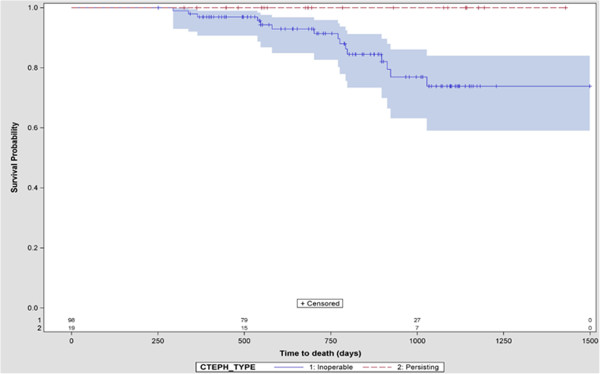
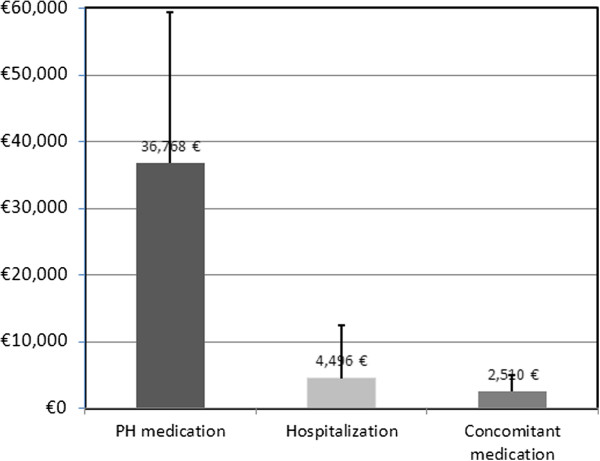
Results: Twenty-one hospitals documented 119 consecutive CTEPH patients over an average of 25.4 months. Patients were inoperable (83.9%) or persistent after surgery (16.0%) with mean age 67.5 ± 12.3 years, 61% were female. The average 6-minute walking distance was 298 ± 120 meters, and NYHA class II/III/IV was 27/59/14%. At baseline, 59.7% patients received endothelin receptor antagonist, 34.4% phosphodiesterase-5 inhibitors, and 5.8% prostacyclin. Adding a second PH medication was the most common regimen change. CTEPH patients experienced 1.8 ± 2.2 hospitalizations per year accounting for 14.8 ± 26.1 days in hospital. Patients paid on average 2.8 office visits per year to their general practitioner and 1.3 visits to a specialist. Unadjusted annual mortality rate was 6.0%. Annual cost of PH specific medication was the predominant economic factor averaging € 36,768 per year. Costs for hospitalizations (€ 4,496) and concomitant medications (€ 2,510) were substantially lower. Other health care resource items only accounted for marginal additional costs.
Conclusion: CTEPH patients are characterised by substantial morbidity and mortality. Health care utilisation, predominantly due to off-label use of PH drugs, is significant.
Figures
References
-
- Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G, Vahanian A, Auricchio A, Bax J, Ceconi C, Dean V, Filippatos G, Funck-Brentano C, Hobbs R, Kearney P, McDonagh T, McGregor K, Popescu BA. et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: The Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT) Eur Heart J. 2009;14:2493–2537. - PubMed
-
- Mehta S, Helmersen D, Provencher S, Hirani N, Rubens FD, De Perrot M, Blostein M, Boutet K, Chandy G, Dennie C, Granton J, Hernandez P, Hirsch AM, Laframboise K, Levy RD, Lien D, Martel S, Shoemaker G, Swiston J, Weinkauf J. Diagnostic evaluation and management of chronic thromboembolic pulmonary hypertension: a clinical practice guideline. Can Respir J. 2010;14:301–334. - PMC - PubMed
-
- Korkmaz AN, Colak MO, Vural C. Pulmonary plasmacytoma, incidentally detected by myocardial perfusion scintigraphy. J Nucl Cardiol. 2012;14:1083–1084. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
