

Review
doi: 10.1182/blood-2014-01-514752.
Epub 2014 Jun 9.
Current issues in chronic graft-versus-host disease
Affiliations
- PMID: 24914139
- PMCID: PMC4102710
- DOI: 10.1182/blood-2014-01-514752
Item in Clipboard
Review
Current issues in chronic graft-versus-host disease
Blood.
.
Abstract
Chronic graft-versus-host disease (GVHD) is a frequent and potentially life-threatening complication of allogeneic hematopoietic stem cell transplantation. Increased transplantation of older patients and the more frequent use of unrelated donors has led to increased numbers of patients with this painful complication. Recent advances have been made in understanding the pathophysiology of chronic GVHD and in establishing precise criteria for diagnosis and classification of disease manifestations. These advances will hopefully pave the way for improving both the prophylaxis and treatment of chronic GVHD.
© 2014 by The American Society of Hematology.
Figures
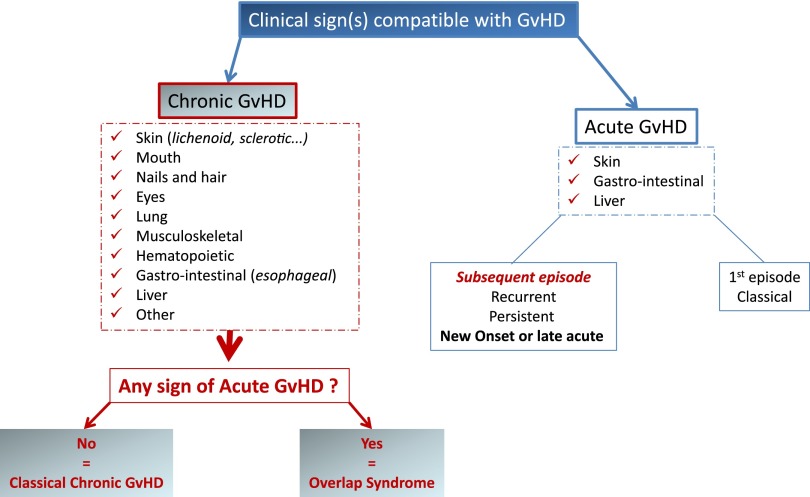
Diagnosis of chronic GVHD according to the NIH consensus criteria.
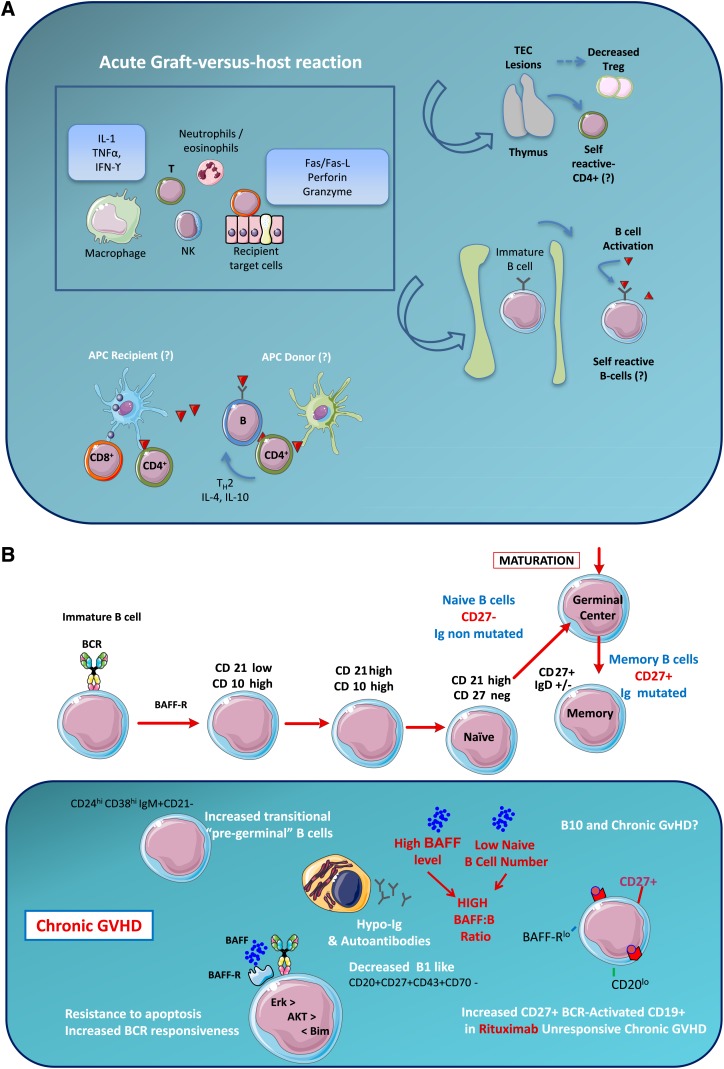
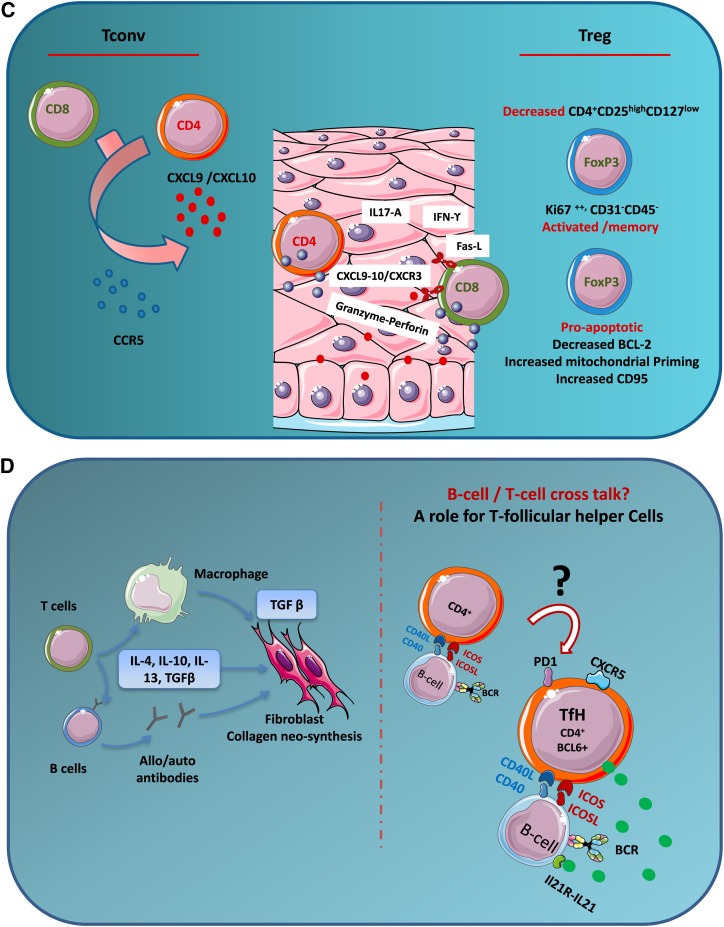
The pathophysiology of chronic GVHD. (A) General mechanisms. The acute graft-versus-host reaction is characterized by tissue damage mediated by inflammatory mediators, T cells, and cells from the innate immune system. Among target organs, two are particularly important for the development of subsequent chronic GVHD: (1) thymic epithelial cells (TECs) are damaged by alloreactive T cells leading to decreased generation of natural Tregs and release of self-reactive T cells. (2) Bone marrow microenvironment damage may explain disturbed B-cell homeostasis. The potent role of antigen-presenting cells (APCs) and the cross talk between B and T cells in chronic GVHD is poorly understood. (B) B cells and chronic GVHD. Patients with chronic GVHD have increased B-cell activation factor (BAFF):B-cell ratios, delayed reconstitution of naive B cells, and increased numbers of pregerminal center B cells. Patients with active chronic GVHD have elevated numbers of CD21– transitional B cells and a deficiency of memory CD27+ B cells. Patients who develop chronic GVHD have elevated levels of BAFF, a relative reduction in naive B cells, and relatively higher numbers of activated memory type B cells. Patients with hypogammaglobulinemia have elevated CD19+CD21low (immature) and CD19+CD21highCD38highIgMhigh (transitional) B cells. CD19+CD10–CD27–CD21high naive B cells are elevated in all patients with chronic GVHD. (C) Conventional T cells, Tregs, and chronic GVHD. An appropriate balance between Tregs and Tconv is critical for the maintenance of peripheral tolerance. In the setting of allogeneic HSCT, Tregs have been shown to play an important role in the establishment of tolerance between recipient tissues and donor-derived immunity. Monitoring of CD4+ T-cell subsets shows that Tregs rapidly expand after HSCT, but Treg levels subsequently decline in patients with prolonged CD4+ lymphopenia. This results in a relative deficiency of Tregs, which is associated with a high incidence of extensive chronic GVHD. In chronic lichenoid GVHD, a mixed Th1/Th17 signature with upregulated Th1/Th17 cytokine/chemokine transcripts and elevated numbers of interferon gamma (IFN-γ)– and IL-17–producing CD8+ T cells has been described. (D) Current issues in chronic GVHD pathophysiology. The hallmark of chronic GVHD is inflammatory fibrosis; putative mechanisms are described in the left part of the figure. Although a role of B- and T-cell subsets has been described, the cross talk between B and T cells is not well understood. Recent evidence from an experimental model suggests that a key player might be the T-follicular helper (TfH) cells. ICOS, inducible costimulatory [molecule]; NK, natural killer [cell]; TGFβ, transforming growth factor beta; TNFα, tumor necrosis factor alpha.
The pathophysiology of chronic GVHD. (A) General mechanisms. The acute graft-versus-host reaction is characterized by tissue damage mediated by inflammatory mediators, T cells, and cells from the innate immune system. Among target organs, two are particularly important for the development of subsequent chronic GVHD: (1) thymic epithelial cells (TECs) are damaged by alloreactive T cells leading to decreased generation of natural Tregs and release of self-reactive T cells. (2) Bone marrow microenvironment damage may explain disturbed B-cell homeostasis. The potent role of antigen-presenting cells (APCs) and the cross talk between B and T cells in chronic GVHD is poorly understood. (B) B cells and chronic GVHD. Patients with chronic GVHD have increased B-cell activation factor (BAFF):B-cell ratios, delayed reconstitution of naive B cells, and increased numbers of pregerminal center B cells. Patients with active chronic GVHD have elevated numbers of CD21– transitional B cells and a deficiency of memory CD27+ B cells. Patients who develop chronic GVHD have elevated levels of BAFF, a relative reduction in naive B cells, and relatively higher numbers of activated memory type B cells. Patients with hypogammaglobulinemia have elevated CD19+CD21low (immature) and CD19+CD21highCD38highIgMhigh (transitional) B cells. CD19+CD10–CD27–CD21high naive B cells are elevated in all patients with chronic GVHD. (C) Conventional T cells, Tregs, and chronic GVHD. An appropriate balance between Tregs and Tconv is critical for the maintenance of peripheral tolerance. In the setting of allogeneic HSCT, Tregs have been shown to play an important role in the establishment of tolerance between recipient tissues and donor-derived immunity. Monitoring of CD4+ T-cell subsets shows that Tregs rapidly expand after HSCT, but Treg levels subsequently decline in patients with prolonged CD4+ lymphopenia. This results in a relative deficiency of Tregs, which is associated with a high incidence of extensive chronic GVHD. In chronic lichenoid GVHD, a mixed Th1/Th17 signature with upregulated Th1/Th17 cytokine/chemokine transcripts and elevated numbers of interferon gamma (IFN-γ)– and IL-17–producing CD8+ T cells has been described. (D) Current issues in chronic GVHD pathophysiology. The hallmark of chronic GVHD is inflammatory fibrosis; putative mechanisms are described in the left part of the figure. Although a role of B- and T-cell subsets has been described, the cross talk between B and T cells is not well understood. Recent evidence from an experimental model suggests that a key player might be the T-follicular helper (TfH) cells. ICOS, inducible costimulatory [molecule]; NK, natural killer [cell]; TGFβ, transforming growth factor beta; TNFα, tumor necrosis factor alpha.
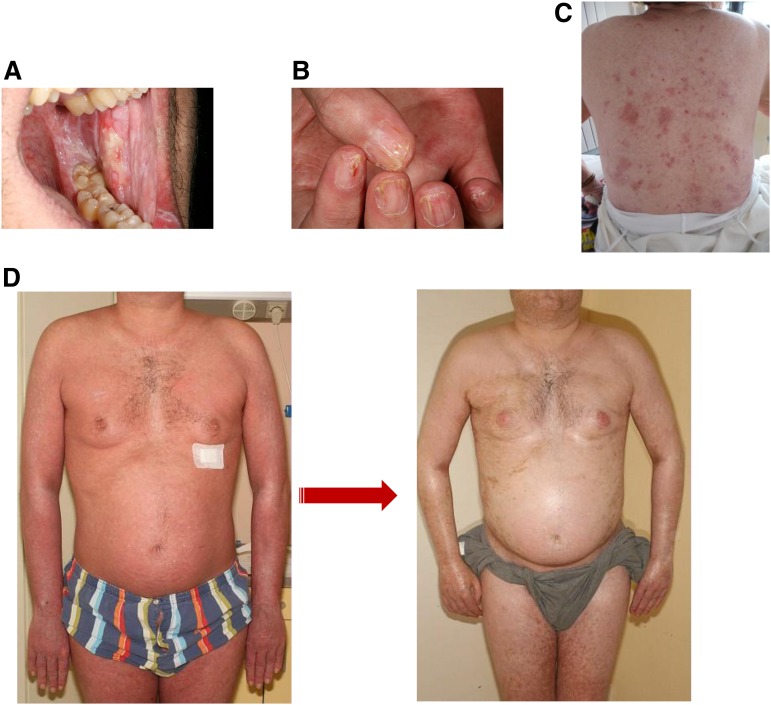
Clinical images of chronic GVHD. (A) Lichen planus-like lesions on buccal mucosa showing a lacework of white streaks and erosions. (B) Lichen planus lesions of the nails showing thinning of the nail plate, longitudinal lines, and pterygium formation. (C) Skin lichen planus lesions with shiny and violaceous papules of the back. (D) Edematous erythroderma with lichenoid features evolving into diffuse sclerodermatous changes of the skin.
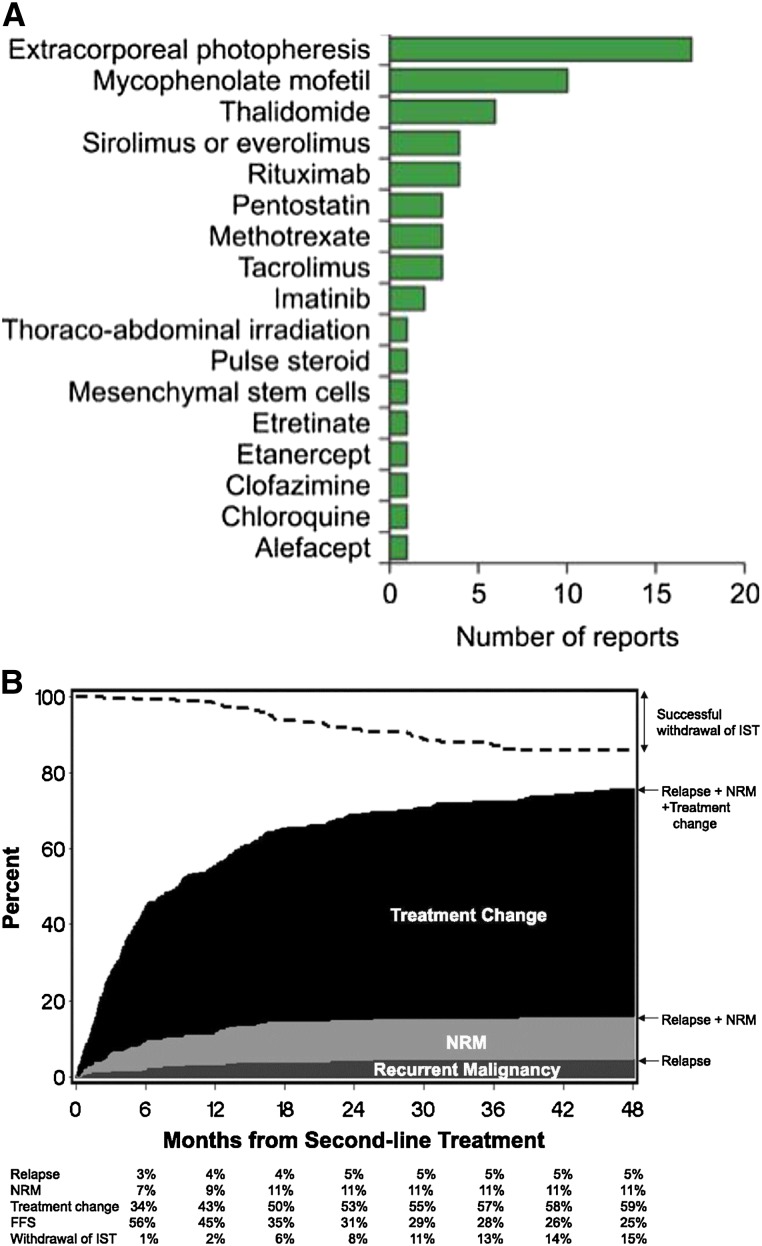
Second-line treatment of chronic GVHD. (A) Number of reports on second-line treatment of chronic GVHD (reprinted with permission from Martin et al). (B) Failure-free survival after second-line treatment of chronic GVHD (reprinted with permission from Inamoto et al). FFS, failure-free survival; IST, immunosuppressive therapy.
References
-
- Socié G, Stone JV, Wingard JR, et al. Late Effects Working Committee of the International Bone Marrow Transplant Registry. Long-term survival and late deaths after allogeneic bone marrow transplantation. N Engl J Med. 1999;341(1):14–21. - PubMed
-
- Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–956. - PubMed
-
- Shulman HM, Kleiner D, Lee SJ, et al. Histopathologic diagnosis of chronic graft-versus-host disease: National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: II. Pathology Working Group Report. Biol Blood Marrow Transplant. 2006;12(1):31–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
