

Conditioning regimens for hematopoietic cell transplantation: one size does not fit all
- PMID: 24914142
- PMCID: PMC4102707
- DOI: 10.1182/blood-2014-02-514778
Conditioning regimens for hematopoietic cell transplantation: one size does not fit all
Abstract
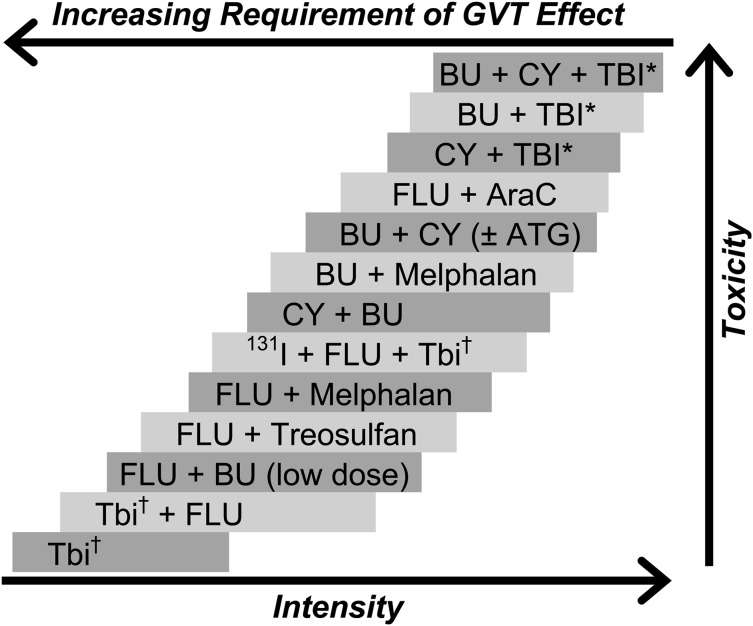
An essential component of allogeneic and autologous hematopoietic cell transplantation (HCT) is the conditioning regimen administered before the hematopoietic cell infusion. Early regimens relied on dose intensity, assuming that high-dose chemoradiotherapy would eliminate malignant disease and reinfusion of the graft would then restore hematopoiesis. However, as the contribution of graft-versus-tumor effects to the success of allogeneic HCT was recognized over time, in an effort to exploit these, many investigators lowered the dose of radiation and chemotherapeutic agents in the preparative regimen. This resulted in a major paradigm shift, and consequently, the pool of eligible patients underwent a remarkable expansion. In this article, we provide a review of the definition of high-dose, reduced-intensity, and nonmyeloablative conditioning regimens, the most commonly used agents and combinations, and the evolution of some early regimens. We also provide a brief review of the toxicities associated with these regimens.
© 2014 by The American Society of Hematology.
Figures
References
-
- Grunebaum E, Mazzolari E, Porta F, et al. Bone marrow transplantation for severe combined immune deficiency. JAMA. 2006;295(5):508–518. - PubMed
-
- Thomas ED, Clift RA, Hersman J, et al. Marrow transplantation for acute nonlymphoblastic leukemic in first remission using fractionated or single-dose irradiation. Int J Radiat Oncol Biol Phys. 1982;8(5):817–821. - PubMed
-
- Brochstein JA, Kernan NA, Groshen S, et al. Allogeneic bone marrow transplantation after hyperfractionated total-body irradiation and cyclophosphamide in children with acute leukemia. N Engl J Med. 1987;317(26):1618–1624. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
