

Outpatient parenteral antimicrobial therapy practices among adult infectious disease physicians
- PMID: 24915212
- PMCID: PMC4180108
- DOI: 10.1086/676859
Outpatient parenteral antimicrobial therapy practices among adult infectious disease physicians
Abstract
Objective: To identify current outpatient parenteral antibiotic therapy practice patterns and complications.
Methods: We administered an 11-question survey to adult infectious disease physicians participating in the Emerging Infections Network (EIN), a Centers for Disease Control and Prevention-sponsored sentinel event surveillance network in North America. The survey was distributed electronically or via facsimile in November and December 2012. Respondent demographic characteristics were obtained from EIN enrollment data.
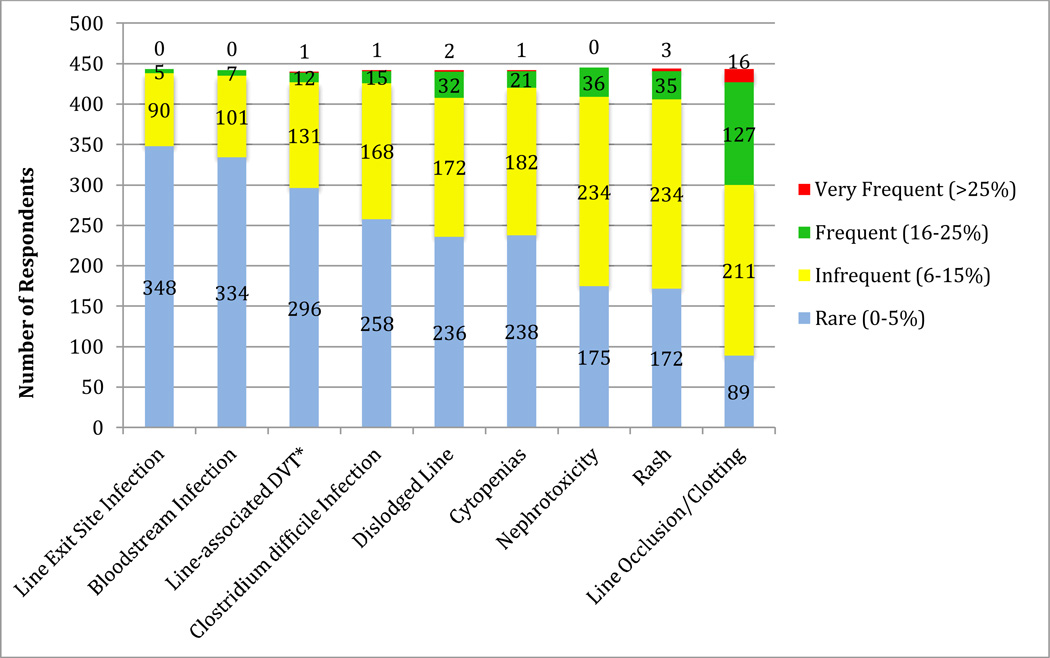
Results: Overall, 555 (44.6%) of EIN members responded to the survey, with 450 (81%) indicating that they treated 1 or more patients with outpatient parenteral antimicrobial therapy (OPAT) during an average month. Infectious diseases consultation was reported to be required for a patient to be discharged with OPAT by 99 respondents (22%). Inpatient (282 [63%] of 449) and outpatient (232 [52%] of 449) infectious diseases physicians were frequently identified as being responsible for monitoring laboratory results. Only 26% (118 of 448) had dedicated OPAT teams at their clinical site. Few infectious diseases physicians have systems to track errors, adverse events, or "near misses" associated with OPAT (97 [22%] of 449). OPAT-associated complications were perceived to be rare. Among respondents, 80% reported line occlusion or clotting as the most common complication (occurring in 6% of patients or more), followed by nephrotoxicity and rash (each reported by 61%). Weekly laboratory monitoring of patients who received vancomycin was reported by 77% of respondents (343 of 445), whereas 19% of respondents (84 of 445) reported twice weekly laboratory monitoring for these patients.
Conclusions: Although use of OPAT is common, there is significant variation in practice patterns. More uniform OPAT practices may enhance patient safety.
Conflict of interest statement
Figures
References
-
- Leder K, Turnidge JD, Grayson ML. Home-based treatment of cellulitis with twice-daily cefazolin. The Medical journal of Australia. 1998;169(10):519–522. - PubMed
-
- Nathwani D. The management of skin and soft tissue infections: outpatient parenteral antibiotic therapy in the United Kingdom. Chemotherapy. 2001;47(Suppl 1):17–23. - PubMed
-
- Eron LJ, Goldenberg RI, Poretz DM. Combined ceftriaxone and surgical therapy for osteomyelitis in hospital and outpatient settings. Am J Surg. 1984;148(4A):1–4. - PubMed
-
- Tice AD. Outpatient parenteral antimicrobial therapy for osteomyelitis. Infect Dis Clin North Am. 1998;12(4):903–919. - PubMed
-
- Esposito S, Noviello S, Leone S, et al. Outpatient parenteral antibiotic therapy (OPAT) in different countries: a comparison. Int J Antimicrob Agents. 2004;24(5):473–478. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- L30 AR063363/AR/NIAMS NIH HHS/United States
- K12 HD001459/HD/NICHD NIH HHS/United States
- U54 CK000162/CK/NCEZID CDC HHS/United States
- KL2 RR024994/RR/NCRR NIH HHS/United States
- KM1CA156708/CA/NCI NIH HHS/United States
- KM1 CA156708/CA/NCI NIH HHS/United States
- KL2 TR000136/TR/NCATS NIH HHS/United States
- UL1RR024992/RR/NCRR NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- KL2RR024994/RR/NCRR NIH HHS/United States
- 1U50CK000187/CK/NCEZID CDC HHS/United States
- CU54 CK 000162/CK/NCEZID CDC HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- 5K12HD001459-13/HD/NICHD NIH HHS/United States
- U50 CK000187/CK/NCEZID CDC HHS/United States
- KL2 TR000450/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical