

Surgical site infections following coronary artery bypass graft procedures: 10 years of surveillance data
- PMID: 24916690
- PMCID: PMC4061097
- DOI: 10.1186/1471-2334-14-318
Surgical site infections following coronary artery bypass graft procedures: 10 years of surveillance data
Abstract
Background: Surgical site infections following coronary artery bypass graft (CABG) procedures pose substantial burden on patients and healthcare systems. This study aims to describe the incidence of surgical site infections and causative pathogens following CABG surgery over the period 2003-2012, and to identify risk factors for complex sternal site infections.
Methods: Routine computerised surveillance data were collected from three public hospitals in Queensland, Australia in which CABG surgery was performed between 2003 and 2012. Surgical site infection rates were calculated by types of infection (superficial/complex) and incision sites (sternal/harvest sites). Patient and procedural characteristics were evaluated as risk factors for complex sternal site infections using a logistic regression model.
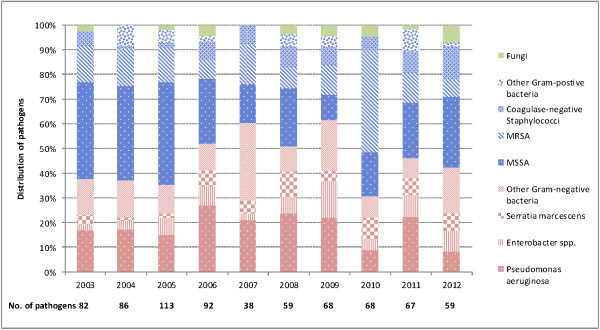
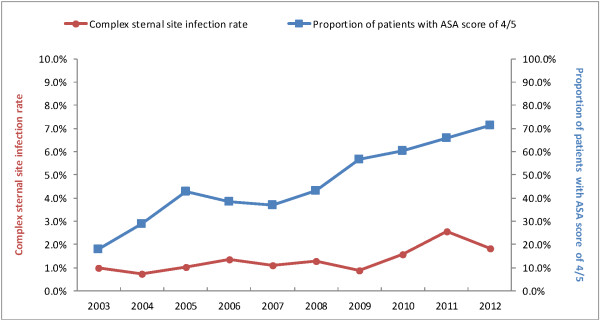
Results: There were 1,702 surgical site infections (518 at sternal sites and 1,184 at harvest sites) following 14,546 CABG procedures performed. Among 732 pathogens isolated, Methicillin-sensitive Staphylococcus aureus accounted for 28.3% of the isolates, Pseudomonas aeruginosa 18.3%, methicillin-resistant Staphylococcus aureus 14.6%, and Enterobacter species 6.7%. Proportions of Gram-negative bacteria elevated from 37.8% in 2003 to 61.8% in 2009, followed by a reduction to 42.4% in 2012. Crude rates of complex sternal site infections increased over the reporting period, ranging from 0.7% in 2004 to 2.6% in 2011. Two factors associated with increased risk of complex sternal site infections were identified: patients with an ASA (American Society of Anaesthesiologists) score of 4 or 5 (reference score of 3, OR 1.83, 95% CI 1.36-2.47) and absence of documentation of antibiotic prophylaxis (OR 2.03, 95% CI 1.12-3.69).
Conclusions: Compared with previous studies, our data indicate the importance of Gram-negative organisms as causative agents for surgical site infections following CABG surgery. An increase in complex sternal site infection rates can be partially explained by the increasing proportion of patients with more severe underlying disease.
Figures
References
-
- Mayhall CG. Hospital Epidemiology and Infection Control. 3. Philadelphia: Lippincott Williams & Wilkins; 2004.
-
- Cruickshank M, Ferguson J. Reducing Harm to Patients from Health Care Associated Infection: The Role of Surveillance. Canberra: Australian Commission on Safety and Quality in Health Care; 2008.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
