

Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis
- PMID: 24917641
- PMCID: PMC4352209
- DOI: 10.1093/eurheartj/ehu218
Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis
Abstract
Aim: Thrombolytic therapy induces faster clot dissolution than anticoagulation in patients with acute pulmonary embolism (PE) but is associated with an increased risk of haemorrhage. We reviewed the risks and benefits of thrombolytic therapy in the management of patients with acute PE.
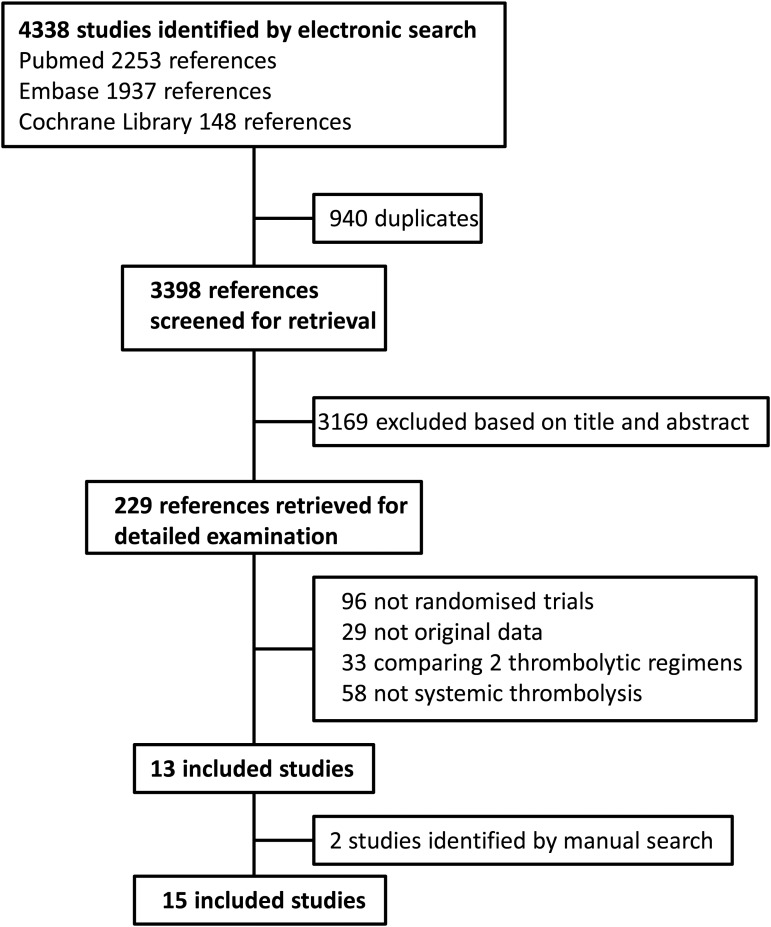
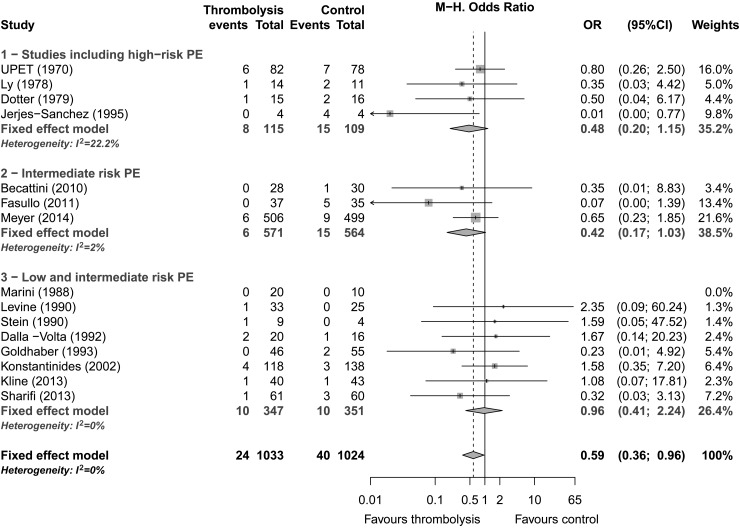
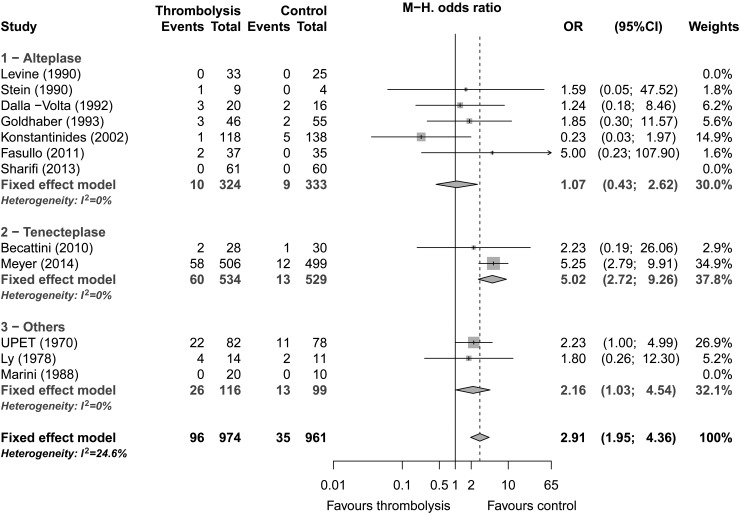
Methods and results: We systematically reviewed randomized controlled studies comparing systemic thrombolytic therapy plus anticoagulation with anticoagulation alone in patients with acute PE. Fifteen trials involving 2057 patients were included in our meta-analysis. Compared with heparin, thrombolytic therapy was associated with a significant reduction of overall mortality (OR; 0.59, 95% CI: 0.36-0.96). This reduction was not statistically significant after exclusion of studies including high-risk PE (OR; 0.64, 95% CI: 0.35-1.17). Thrombolytic therapy was associated with a significant reduction in the combined endpoint of death or treatment escalation (OR: 0.34, 95% CI: 0.22-0.53), PE-related mortality (OR: 0.29; 95% CI: 0.14-0.60) and PE recurrence (OR: 0.50; 95% CI: 0.27-0.94). Major haemorrhage (OR; 2.91, 95% CI: 1.95-4.36) and fatal or intracranial bleeding (OR: 3.18, 95% CI: 1.25-8.11) were significantly more frequent among patients receiving thrombolysis.
Conclusions: Thrombolytic therapy reduces total mortality, PE recurrence, and PE-related mortality in patients with acute PE. The decrease in overall mortality is, however, not significant in haemodynamically stable patients with acute PE. Thrombolytic therapy is associated with an increase of major and fatal or intracranial haemorrhage.
Keywords: Pulmonary embolism; Systematic review; Thrombolytic therapy.
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Kroger K, Moerchel C, Moysidis T, Santosa F. Incidence rate of pulmonary embolism in Germany: data from the federal statistical office. J Thromb Thrombolysis. 2010;29:349–353. - PubMed
-
- Laporte S, Mismetti P, Decousus H, Uresandi F, Otero R, Lobo JL, Monreal M. Clinical predictors for fatal pulmonary embolism in 15,520 patients with venous thromboembolism: findings from the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) Registry. Circulation. 2008;117:1711–1716. - PubMed
-
- Aujesky D, Hughes R, Jimenez D. Short-term prognosis of pulmonary embolism. J Thromb Haemost. 2009;7(Suppl. 1):318–321. - PubMed
-
- Stein PD, Kayali F, Olson RE. Estimated case fatality rate of pulmonary embolism, 1979 to 1998. Am J Cardiol. 2004;93:1197–1199. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
