

The effect of Helicobacter pylori infection and eradication in patients with gastro-oesophageal reflux disease: A parallel-group, double-blind, placebo-controlled multicentre study
- PMID: 24917966
- PMCID: PMC4040789
- DOI: 10.1177/2050640613484020
The effect of Helicobacter pylori infection and eradication in patients with gastro-oesophageal reflux disease: A parallel-group, double-blind, placebo-controlled multicentre study
Abstract
Objectives: This study aimed to resolve controversy regarding the effects of Helicobacter pylori eradication therapy and H. pylori infection in gastro-oesophageal reflux disease.
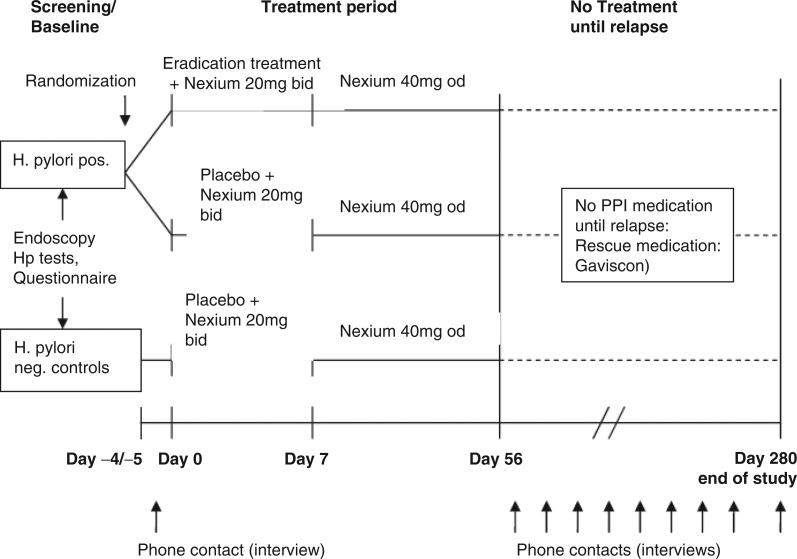
Design: A randomized, double-blind, multicentre trial was performed in patients presenting with reflux symptoms. H. pylori-positive patients were randomized to receive either antibiotics or placebo for 7 days. H. pylori-negative patient controls received placebo. All received esomeprazole 20 mg b.d. for 7 days, followed by 40 mg o.d. to complete an 8-week course, and were followed up for 32 weeks by telephone.
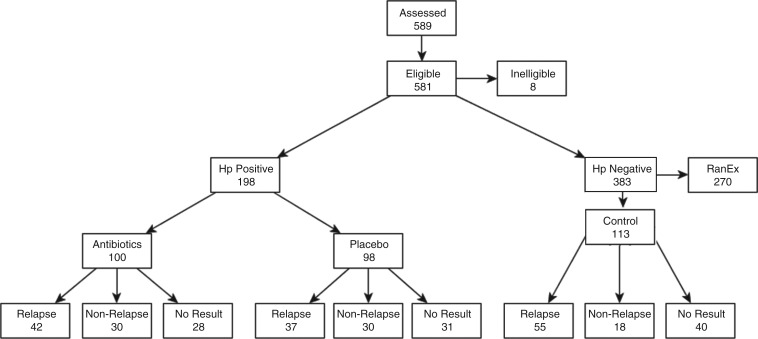
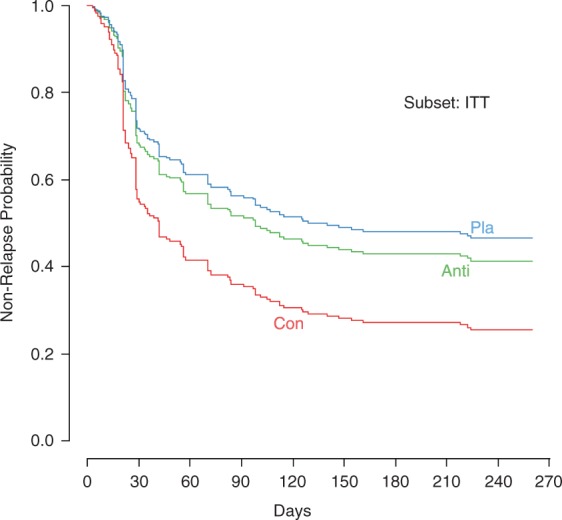
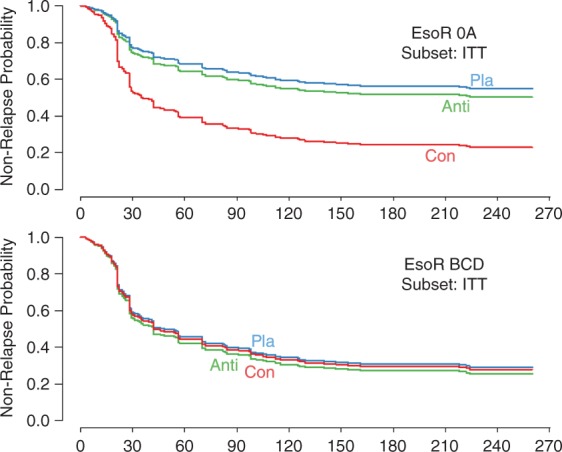
Results: In this study, 198/589 (34%) patients were H. pylori-positive and 113 H. pylori-negative patients served as controls. Baseline endoscopy revealed 63% Los Angeles grade 0A and 37% Los Angeles grade BCD oesophagitis with no difference between patient groups. Symptom improvement on esomeprazole was seen in 89%. H. pylori eradication was successful in 82%. H. pylori eradication had no effect on symptomatic relapse (hazard ratio 1.15, 95% CI 0.74-1.8; p = 0.5). Overall, H. pylori-positive patients had a lower probability of relapse compared to H. pylori-negative controls (hazard ratio 0.6, 95% CI 0.43-0.85; p = 0.004). Relapse hazard was modulated also by oesophagitis grade (BCD vs. 0A, hazard ratio 2.1, 95% CI 1.5-3.0).
Conclusion: Relapse of gastro-oesophageal reflux disease symptoms after a course of high dose acid suppression took longer for H. pylori-positive patients than H. pylori-negative controls; however eradication therapy had no effect on the risk of relapse; ClincialTrials.gov number, NCT00574925.
Keywords: H. pylori eradication therapy; Helicobacter pylori; esomeprazole; gastritis; gastro-oesophageal reflux disease; oesophagitis; symptomatic relapse.
Figures
Similar articles
-
Effect of Helicobacter pylori eradication on treatment of gastro-oesophageal reflux disease: a double blind, placebo controlled, randomised trial.Gut. 2004 Feb;53(2):174-9. doi: 10.1136/gut.2003.012641. Gut. 2004. PMID: 14724146 Free PMC article. Clinical Trial.
-
Helicobacter pylori and symptomatic relapse of gastro-oesophageal reflux disease: a randomised controlled trial.Lancet. 2001 Jun 2;357(9270):1738-42. doi: 10.1016/S0140-6736(00)04894-7. Lancet. 2001. PMID: 11403809 Clinical Trial.
-
Recurrent symptoms and gastro-oesophageal reflux disease in patients with duodenal ulcer treated for Helicobacter pylori infection.Aliment Pharmacol Ther. 2000 Jan;14(1):45-51. doi: 10.1046/j.1365-2036.2000.00677.x. Aliment Pharmacol Ther. 2000. PMID: 10632644 Clinical Trial.
-
Review article: Helicobacter pylori and gastro-oesophageal reflux disease.Aliment Pharmacol Ther. 2005 Aug;22 Suppl 1:32-40. doi: 10.1111/j.1365-2036.2005.02607.x. Aliment Pharmacol Ther. 2005. PMID: 16042657 Review.
-
Omeprazole. A review of its use in Helicobacter pylori infection, gastro-oesophageal reflux disease and peptic ulcers induced by nonsteroidal anti-inflammatory drugs.Drugs. 1998 Sep;56(3):447-86. doi: 10.2165/00003495-199856030-00012. Drugs. 1998. PMID: 9777317 Review.
Cited by
-
Helicobacter pylori Related Diseases and Osteoporotic Fractures (Narrative Review).J Clin Med. 2020 Oct 12;9(10):3253. doi: 10.3390/jcm9103253. J Clin Med. 2020. PMID: 33053671 Free PMC article. Review.
-
Management of Helicobacter pylori infection: The Bhubaneswar Consensus Report of the Indian Society of Gastroenterology.Indian J Gastroenterol. 2021 Aug;40(4):420-444. doi: 10.1007/s12664-021-01186-4. Epub 2021 Jul 5. Indian J Gastroenterol. 2021. PMID: 34219211
-
Dentists Are at a Higher Risk for Oral Helicobacter pylori Infection.Biomed Res Int. 2020 Jul 4;2020:3945189. doi: 10.1155/2020/3945189. eCollection 2020. Biomed Res Int. 2020. PMID: 32695813 Free PMC article.
-
Do we need to eradicate Helicobacter pylori in patients with GORD?United European Gastroenterol J. 2013 Aug;1(4):223-5. doi: 10.1177/2050640613497713. United European Gastroenterol J. 2013. PMID: 24917965 Free PMC article.
-
ACG Clinical Guideline: Treatment of Helicobacter pylori Infection.Am J Gastroenterol. 2017 Feb;112(2):212-239. doi: 10.1038/ajg.2016.563. Epub 2017 Jan 10. Am J Gastroenterol. 2017. PMID: 28071659
References
-
- Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999; 340: 825–831 - PubMed
-
- Kuipers EJ, Uyterlinde AM, Pena AS, et al. Increase of Helicobacter pylori-associated corpus gastritis during acid suppressive therapy: implications for long-term safety. Am J Gastroenterol 1995; 90: 1401–1406 - PubMed
-
- Richter JE, Kahrilas PJ, Johanson J, et al. Efficacy and safety of esomeprazole compared with omeprazole in GERD patients with erosive esophagitis: a randomized controlled trial. Am J Gastroenterol 2001; 96: 656–965 - PubMed
-
- Graham KS, Graham DY. Helicobacter pylori, gastroesophageal reflux disease, Barrett's esophagus, and adenocarcinoma of the distal esophagus. In: Contemporary diagnosis and management of Helicobacter pylori-associated gastrointestinal diseases, 2nd ed Newtown: Pennsylvania, 2002; 128–147
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
