

Factors associated with systemic hypertension in asthma
- PMID: 24920421
- PMCID: PMC4543317
- DOI: 10.1007/s00408-014-9600-y
Factors associated with systemic hypertension in asthma
Abstract
Purpose: Asthmatics have unique characteristics that may influence cardiovascular morbidity. We tested the association of lower airway caliber, obstructive sleep apnea (OSA), and other asthma-related factors, with systemic hypertension (HTN).
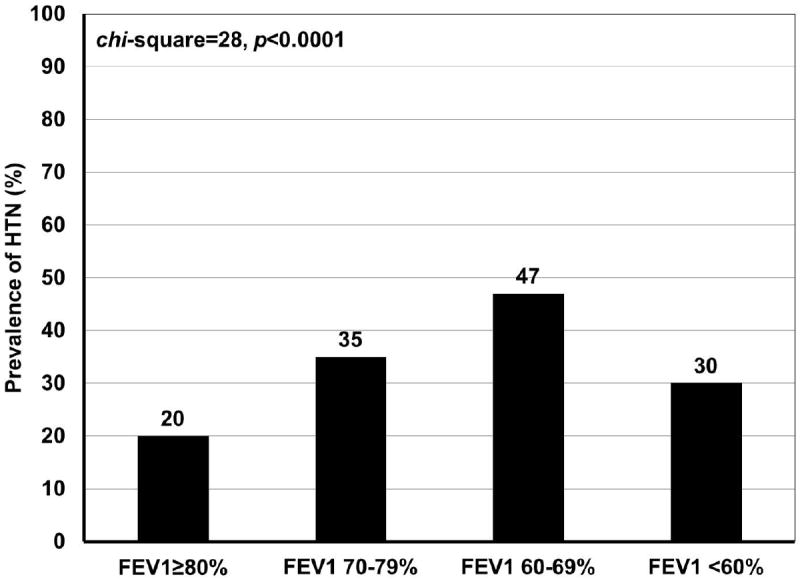
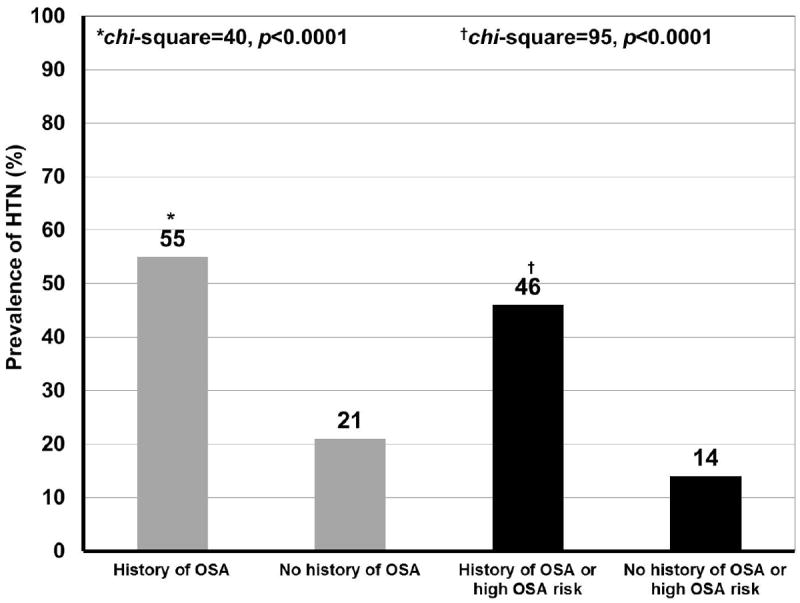
Methods: Asthma individuals at specialty clinics completed the Sleep Apnea scale of the Sleep Disorders Questionnaire (SA-SDQ). Medical records were reviewed for diagnosed HTN, OSA and comorbidities, spirometry, and current medications. FEV1% predicted was categorized as ≥ 80 (reference), 70-79, 60-69, and < 60. SA-SDQ ≥ 36 for men and ≥ 32 for women defined high OSA risk.
Results: Among 812 asthmatics (mean age ± standard deviation: 46 ± 14 years), HTN was diagnosed in 191 (24%), OSA in 65 (8%), and OSA or high OSA risk (combined OSA variable) in 239 (29%). HTN was more prevalent in lower FEV1% categories (p < 0.0001), in subjects with OSA, and those with combined OSA variable (55 vs. 21% and 46 vs. 14%, respectively, both p < 0.0001). With adjustment for covariates, associations with HTN remained significant for some FEV1% categories (70-79% odds ratio = 1.60 [95% CI 0.90-2.87]; 60-69% 2.73 [1.28-5.79]; < 60% 0.96 [0.43-2.14]), and for OSA (2.20 [1.16-4.19]). The combined OSA variable in comparison with OSA alone demonstrated a stronger association with HTN (3.17 [1.99-5.04]) in a reiteration of this model. Inhaled corticosteroids (ICS) at lowest doses, in comparison to no ICS use had an independent "protective" association with HTN (0.44 [0.22-0.90]).
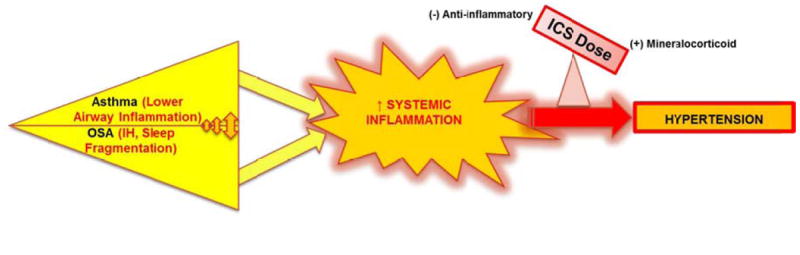
Conclusions: In this young population, worse lower airways obstruction and OSA were associated with HTN. In contrast, lower ICS doses attenuated likelihood for HTN. Adequate control of airway inflammation at appropriate ICS doses, and screening for OSA may reduce the burden of HTN in asthma.
Figures
References
-
- Center for Disease Control and Prevention: National Center for Health Statistics. US Department of Health and Human Services. [April 28, 2013];FastStats. Hypertension 2009-2010. Available at http://www.cdc.gov/nchs/fastats/hyprtens.htm.
-
- Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease (COPD) and asthma. Am Rev Respir Dis. 136(1):225–244. - PubMed
-
- US Department of Health and Human Services. National Institute of Health; National Heart, Lung and Blood Institute. National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3) [April 15, 2013];Guidelines for the Diagnosis and Management of Asthma. Full Report 2007. Available at http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf.
-
- Auckley D, Moallem M, Shaman Z, et al. Findings of a Berlin Questionnaire survey: comparison between patients seen in an asthma clinic versus internal medicine clinic. Sleep Med. 2008;9:494–499. - PubMed
-
- Bettiol J, Bartsch P, Louis R, et al. Cytokine production from peripheral whole blood in atopic and nonatopic asthmatics: relationship with blood and sputum eosinophilia and serum IgE levels. Allergy. 2000;55:1134–1141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
