

Comparative study of Y-split recession versus bilateral medial rectus recession for surgical management of infantile esotropia
- PMID: 24920880
- PMCID: PMC4043800
- DOI: 10.2147/OPTH.S59036
Comparative study of Y-split recession versus bilateral medial rectus recession for surgical management of infantile esotropia
Abstract
Aim: This prospective study compares the results of bilateral medial rectus recession versus (vs) Y-split recession of medial recti techniques for surgical management of essential infantile esotropia.
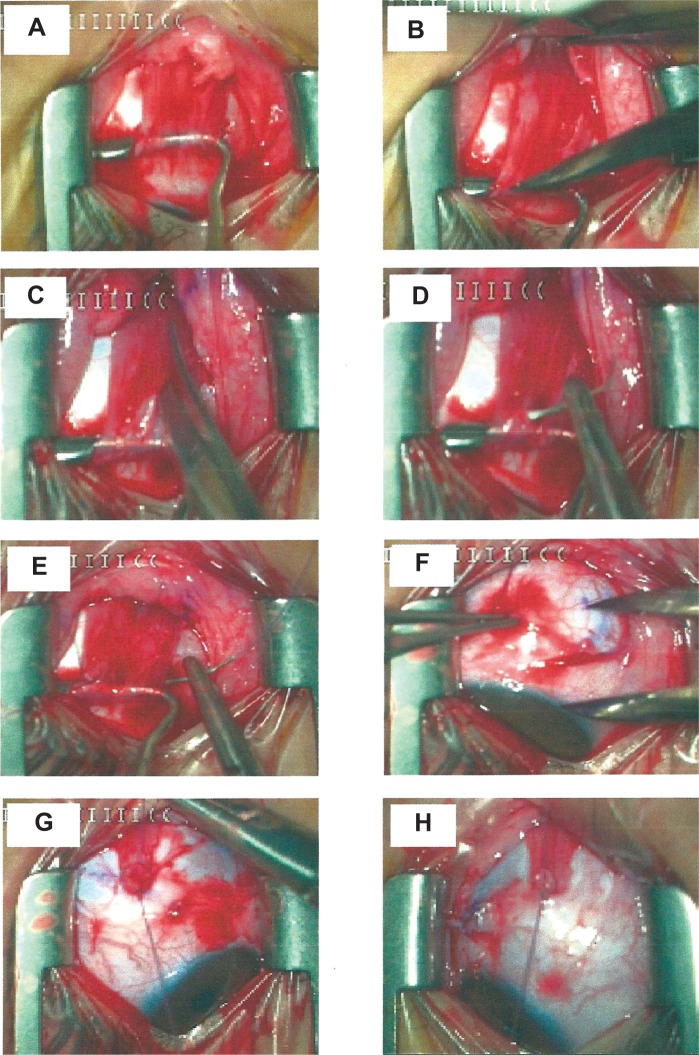
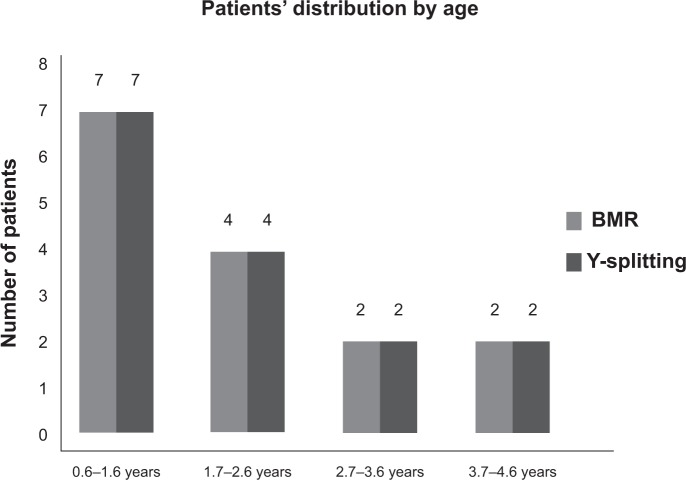
Patients and methods: Thirty patients were included in this study and had preoperative infantile esotropia with large angles (ie, >30 prism diopters [PD]). Patients were divided into Group A, which underwent bilateral medial rectus (BMR) recession and Group B, which underwent bilateral Y-split recession of medial recti muscles. All patients were subjected to complete ophthalmologic examination and met the criteria for inclusion in this study. The degrees of BMR recessions performed ranged from 6.0-7.5 mm. All operations were performed under general anesthesia. Follow-up visits were conducted at 1 and 2 weeks, and 1, 3, and 6 months postoperatively. Rates of reoperation for residual esotropia and consecutive exotropia were determined.
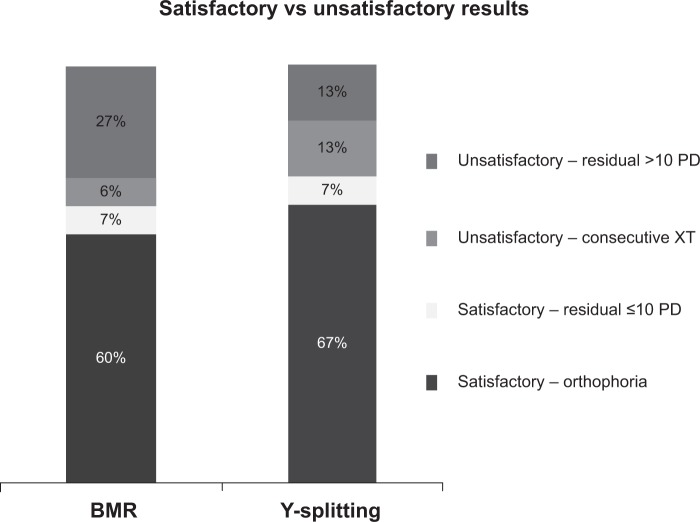
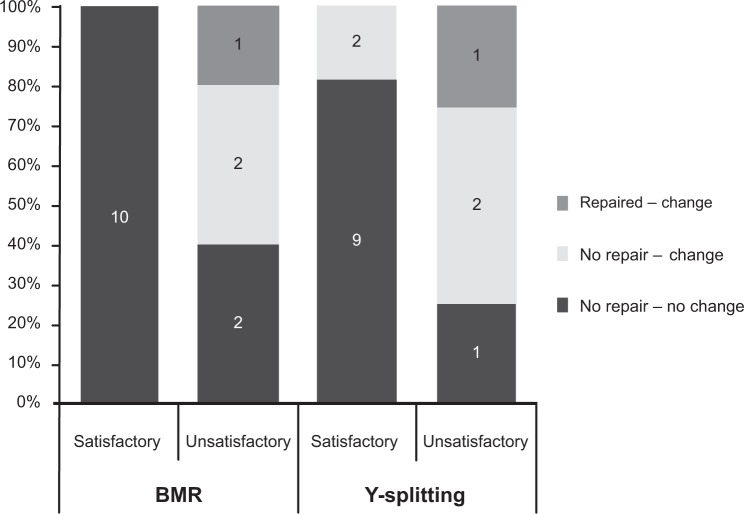
Results: The patients' preoperative angles of deviation ranged from 30-80 PD. Group A consumed 57% less operative time than Group B. Immediately postoperatively, the Y-splitting technique showed satisfactory results (ie, orthotropic or residual angles ≤15 PD) in 73% of patients vs 67% only for the BMR recession patients. By the end of six months of follow up; 13% of the BMR technique patients vs 27% of the Y-splitting technique patients showed negative change of PD but without reoperation.
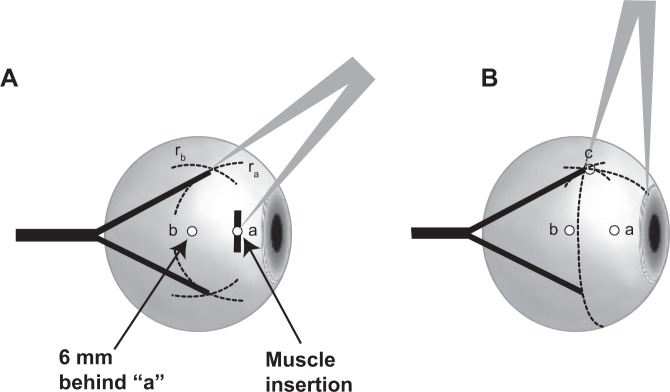
Conclusion: Our results suggest that, although the Y-splitting technique is more difficult and time consuming, both procedures are effective and have shown comparable results for the correction of horizontal deviation ≤70 PD.
Keywords: BMR recession; Y-splitting technique; faden operation; oculomotor pathology; strabismus; torque reduction.
Figures
References
-
- Stager DR, Weakley DR, Jr, Everett M, Birch EE. Delayed consecutive exotropia following 7-millimeter bilateral medial rectus recession for congenital esotropia. J Pediatr Ophthalmol Strabismus. 1994;31(3):147–150. - PubMed
-
- Birch EE, Felius J, Stager DR, Sr, Weakley DR, Jr, Bosworth RG. Preoperative stability of infantile esotropia and post-operative outcome. Am J Ophthalmol. 2004;138(6):1003–1009. - PubMed
-
- Ruiz MF, Alvarez MT, Sánchez-Garrido CM, Hernáez JM, Rodríguez JM. Surgery and botulinum toxin in congenital esotropia. Can J Ophthalmol. 2004;39(6):639–649. - PubMed
-
- Elliott S, Shafiq A. Interventions for infantile esotropia. Cochrane Database Syst Rev. 2005;25(1):CD004917. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
