

Is the pain visual analogue scale linear and responsive to change? An exploration using Rasch analysis
- PMID: 24921952
- PMCID: PMC4055724
- DOI: 10.1371/journal.pone.0099485
Is the pain visual analogue scale linear and responsive to change? An exploration using Rasch analysis
Abstract
Objectives: Pain visual analogue scales (VAS) are commonly used in clinical trials and are often treated as an interval level scale without evidence that this is appropriate. This paper examines the internal construct validity and responsiveness of the pain VAS using Rasch analysis.
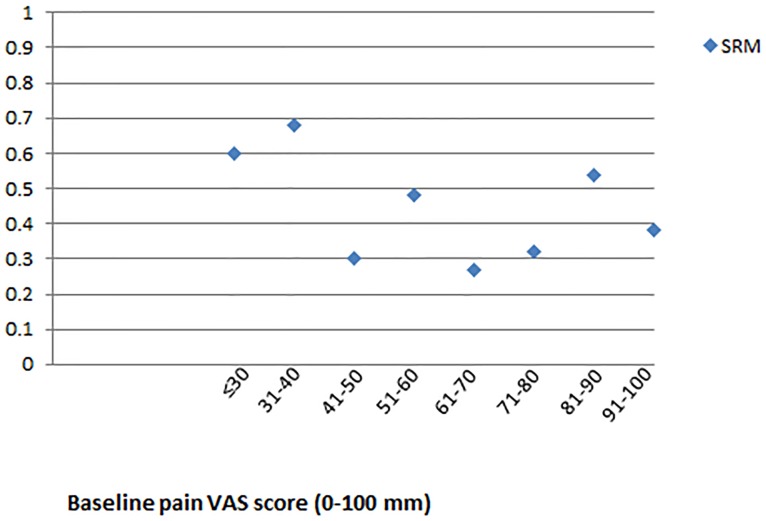
Methods: Patients (n = 221, mean age 67, 58% female) with chronic stable joint pain (hip 40% or knee 60%) of mechanical origin waiting for joint replacement were included. Pain was scored on seven daily VASs. Rasch analysis was used to examine fit to the Rasch model. Responsiveness (Standardized Response Means, SRM) was examined on the raw ordinal data and the interval data generated from the Rasch analysis.
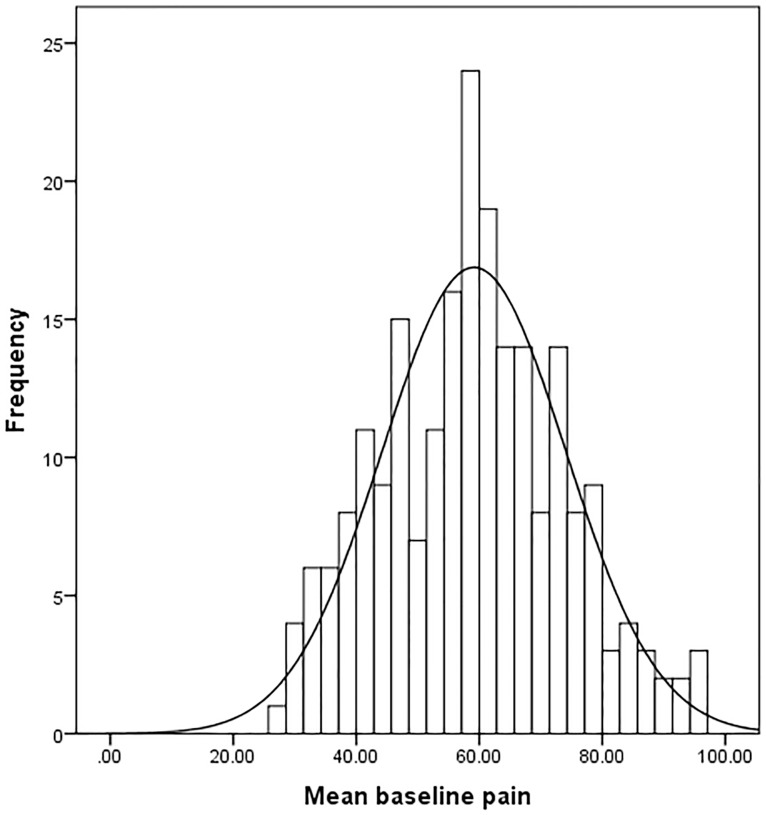
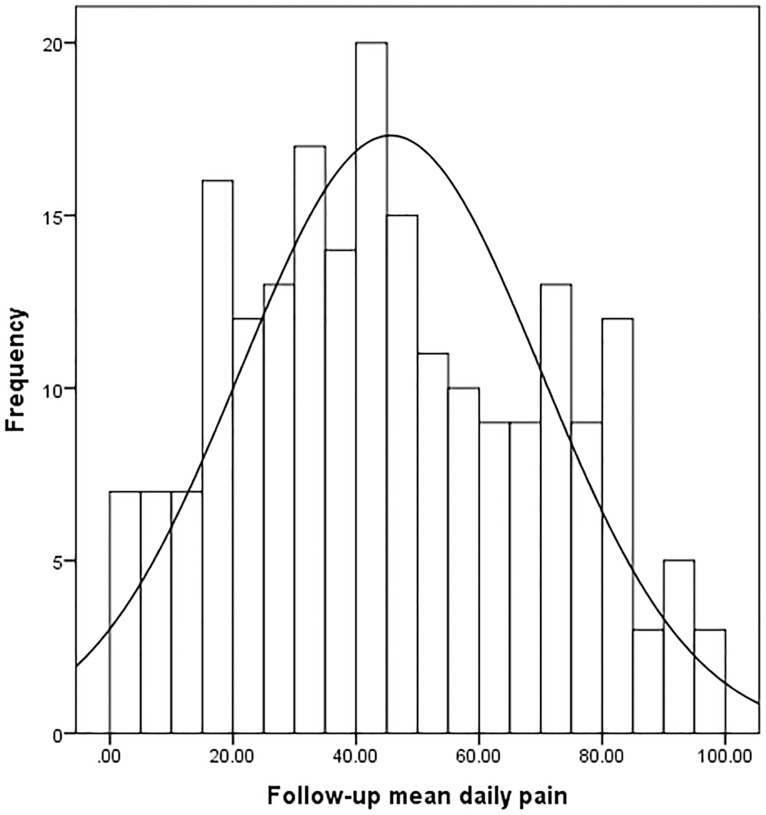
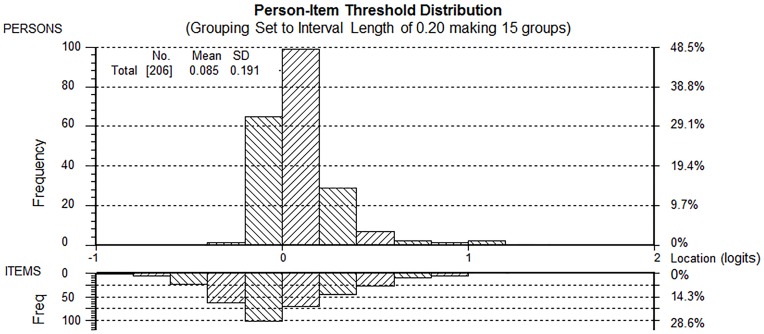
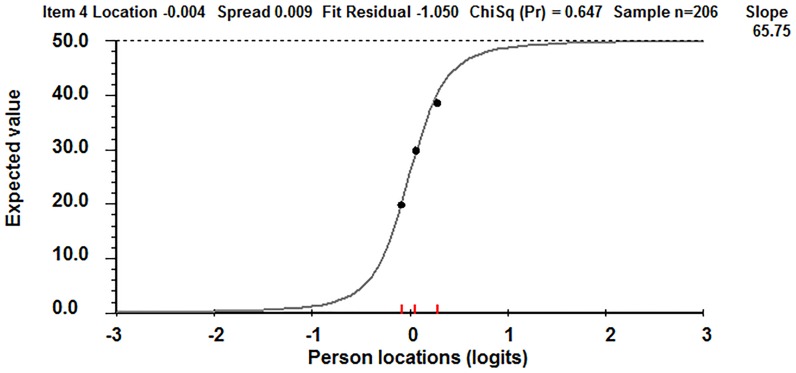
Results: Baseline pain VAS scores fitted the Rasch model, although 15 aberrant cases impacted on unidimensionality. There was some local dependency between items but this did not significantly affect the person estimates of pain. Daily pain (item difficulty) was stable, suggesting that single measures can be used. Overall, the SRMs derived from ordinal data overestimated the true responsiveness by 59%. Changes over time at the lower and higher end of the scale were represented by large jumps in interval equivalent data points; in the middle of the scale the reverse was seen.
Conclusions: The pain VAS is a valid tool for measuring pain at one point in time. However, the pain VAS does not behave linearly and SRMs vary along the trait of pain. Consequently, Minimum Clinically Important Differences using raw data, or change scores in general, are invalid as these will either under- or overestimate true change; raw pain VAS data should not be used as a primary outcome measure or to inform parametric-based Randomised Controlled Trial power calculations in research studies; and Rasch analysis should be used to convert ordinal data to interval data prior to data interpretation.
Conflict of interest statement
Figures
References
-
- Brouwer RW, Bierma-Zeinstra SMA, van Raaij TM, Verhaar JAN (2006) Osteotomy for medial compartment arthritis of the knee using a closing wedge or an opening wedge controlled by a Puddu plate. A one-year randomised, controlled study. J Bone Joint Surg - Series B 88: 1454–1459. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
