

Hospital variation in survival trends for in-hospital cardiac arrest
- PMID: 24922627
- PMCID: PMC4309112
- DOI: 10.1161/JAHA.114.000871
Hospital variation in survival trends for in-hospital cardiac arrest
Abstract
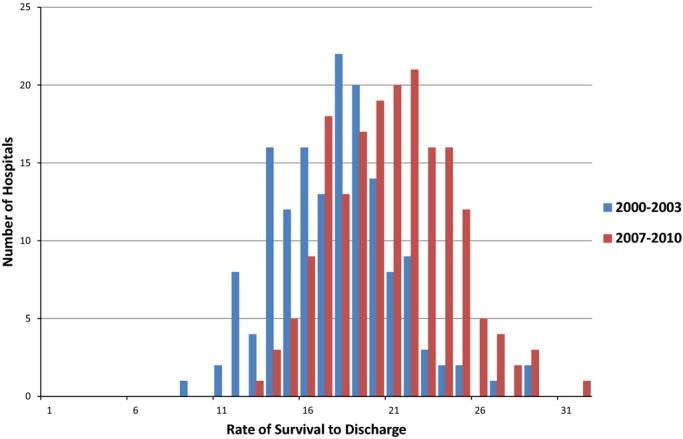
Background: During the past decade, survival after in-hospital cardiac arrest has improved markedly. It remains unknown whether the improvement in survival has occurred uniformly at all hospitals or was driven by large improvements at only a few hospitals.
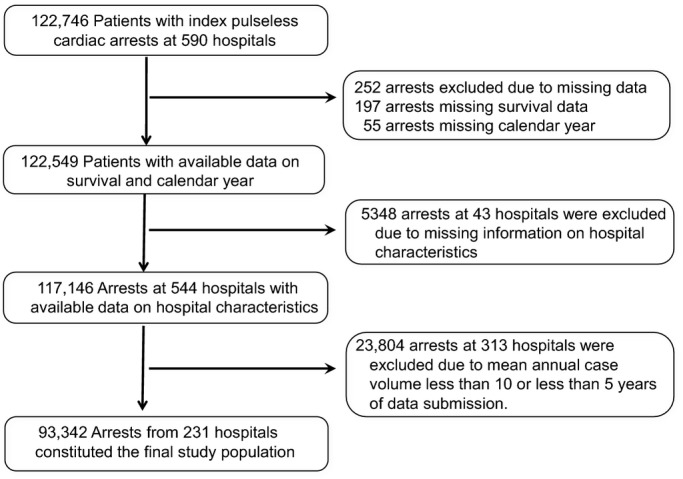
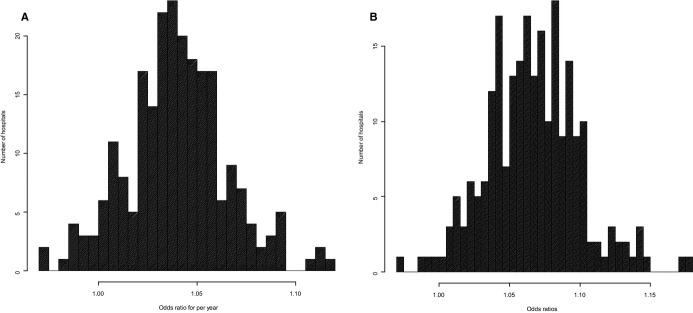
Methods and results: We identified 93 342 adults with an in-hospital cardiac arrest at 231 hospitals in the Get With The Guidelines(®)-Resuscitation registry during 2000-2010. Using hierarchical regression models, we evaluated hospital-level trends in survival to discharge. Mean age was 66 years, 59% were men, and 21% were black. Between 2000 and 2010, there was a significant decrease in age, prevalence of heart failure and myocardial infarction, and cardiac arrests due to shockable rhythms (P<0.001 for all) and an increase in prevalence of sepsis, respiratory insufficiency, renal insufficiency, intensive care unit location, and mechanical ventilation before arrest (P<0.001 for all). After adjustment for temporal trends in baseline characteristics, hospital rates of in-hospital cardiac arrest survival improved by 7% per year (odds ratio [OR] 1.07, 95% CI 1.06 to 1.08, P<0.001). Improvement in survival varied markedly and ranged from 3% in the bottom hospital quartile to 11% in the top hospital quartile. Compared with minor teaching hospitals (OR 1.04, 95% CI 1.02 to 1.06), hospital rate of survival improvement was greater at major teaching (OR 1.08, 95% CI 1.06 to 1.10) and nonteaching hospitals (OR 1.07, 95% CI 1.05 to 1.09, P value for interaction=0.03).
Conclusion: Although in-hospital cardiac arrest survival has improved during the past decade, the magnitude of improvement varied across hospitals. Future studies are needed to identify hospital processes that have led to the largest improvement in survival.
Keywords: cardiac arrest; cardiopulmonary resuscitation; health services research; survival.
© 2014 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Peberdy MA, Kaye W, Ornato JP, Larkin GL, Nadkarni V, Mancini ME, Berg RA, Nichol G, Lane‐Trultt T. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the national registry of cardiopulmonary resuscitation. Resuscitation. 2003; 58:297-308. - PubMed
-
- Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, Cassan P, Coovadia A, D'Este K, Finn J, Halperin H, Handley A, Herlitz J, Hickey R, Idris A, Kloeck W, Larkin GL, Mancini ME, Mason P, Mears G, Monsieurs K, Montgomery W, Morley P, Nichol G, Nolan J, Okada K, Perlman J, Shuster M, Steen PA, Sterz F, Tibballs J, Timerman S, Truitt T, Zideman D. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, Interamerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation. 2004; 110:3385-3397. - PubMed
-
- Cummins RO, Chamberlain D, Hazinski MF, Nadkarni V, Kloeck W, Kramer E, Becker L, Robertson C, Koster R, Zaritsky A, Bossaert L, Ornato JP, Callanan V, Allen M, Steen P, Connolly B, Sanders A, Idris A, Cobbe S. Recommended guidelines for reviewing, reporting, and conducting research on in‐hospital resuscitation: the in‐hospital ‘Utstein style.’ American Heart Association. Circulation. 1997; 95:2213-2239. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
