

Caffeic acid phenethyl amide ameliorates ischemia/reperfusion injury and cardiac dysfunction in streptozotocin-induced diabetic rats
- PMID: 24923878
- PMCID: PMC4065079
- DOI: 10.1186/1475-2840-13-98
Caffeic acid phenethyl amide ameliorates ischemia/reperfusion injury and cardiac dysfunction in streptozotocin-induced diabetic rats
Abstract
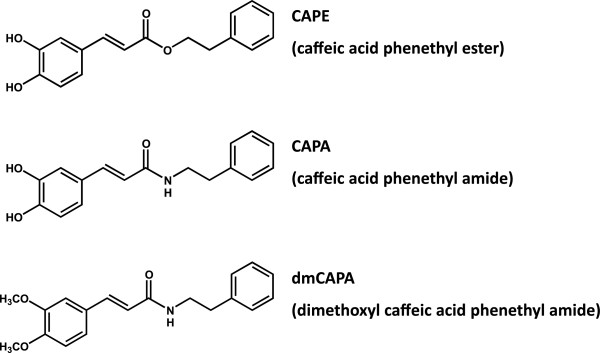
Background: Caffeic acid phenethyl ester (CAPE) has been shown to protect the heart against ischemia/reperfusion (I/R) injury by various mechanisms including its antioxidant effect. In this study, we evaluated the protective effects of a CAPE analog with more structural stability in plasma, caffeic acid phenethyl amide (CAPA), on I/R injury in streptozotocin (STZ)-induced type 1 diabetic rats.
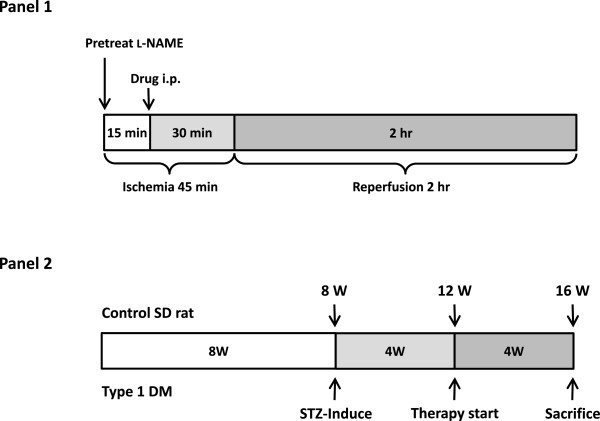
Methods: Type 1 diabetes mellitus was induced in Sprague-Dawley rats by a single intravenous injection of 60 mg/kg STZ. To produce the I/R injury, the left anterior descending coronary artery was occluded for 45 minutes, followed by 2 hours of reperfusion. CAPA was pretreated intraperitoneally 30 minutes before reperfusion. An analog devoid of the antioxidant property of CAPA, dimethoxyl CAPA (dmCAPA), and a nitric oxide synthase (NOS) inhibitor (Nω-nitro-l-arginine methyl ester [l-NAME]) were used to evaluate the mechanism involved in the reduction of the infarct size following CAPA-treatment. Finally, the cardioprotective effect of chronic treatment of CAPA was analyzed in diabetic rats.
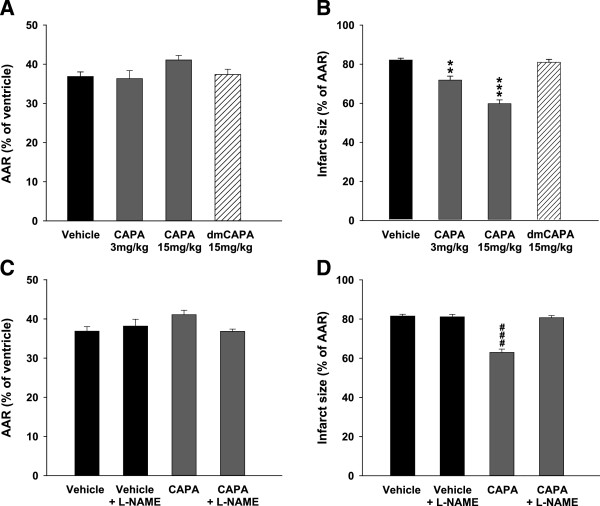
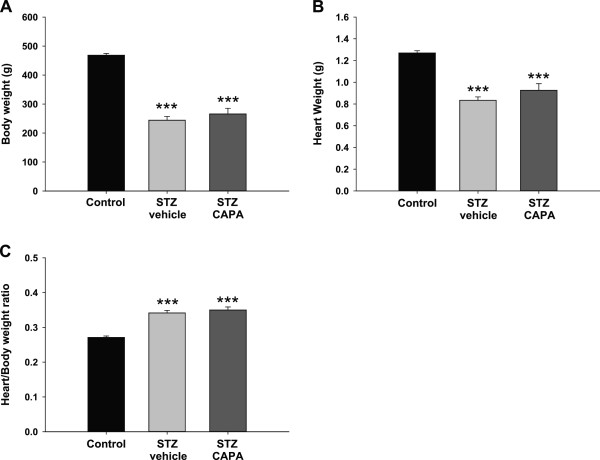
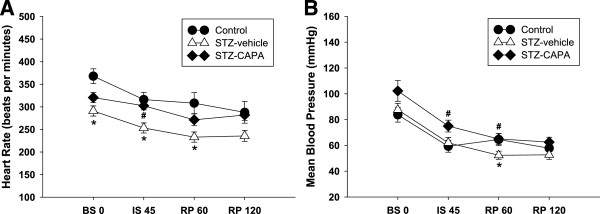
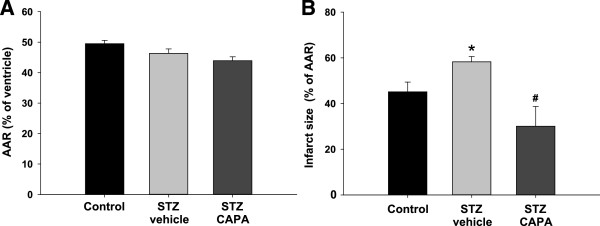
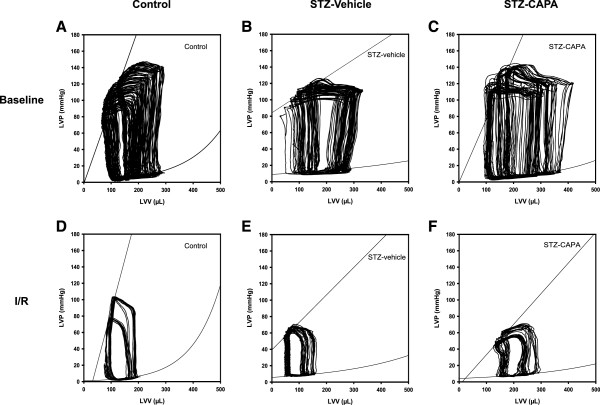
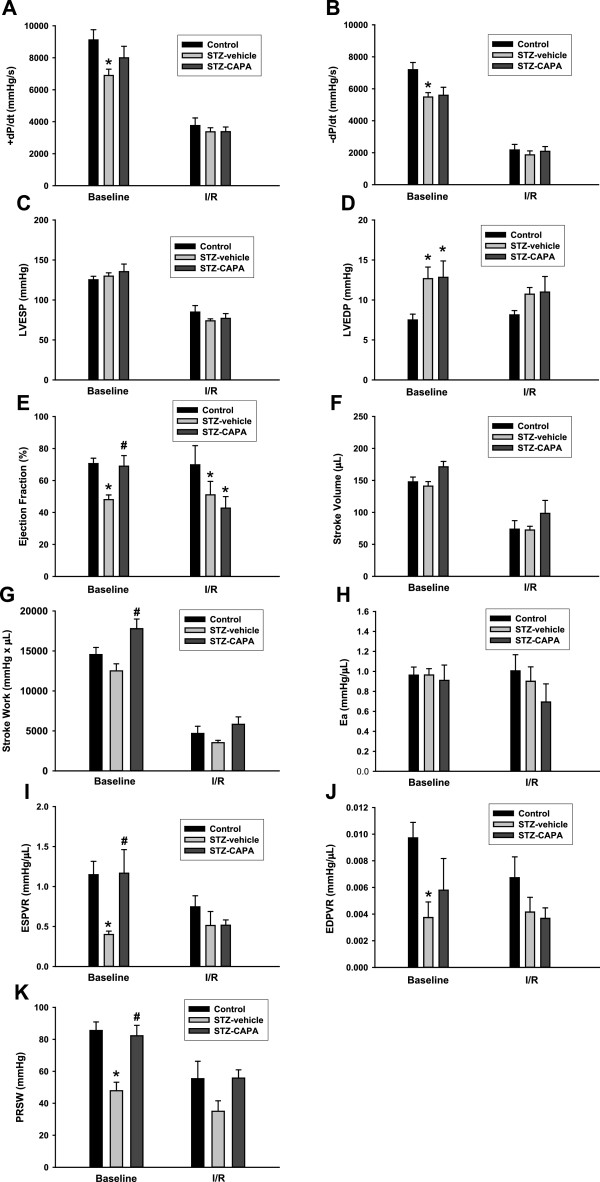
Results: Compared to the control group, CAPA administration (3 and 15 mg/kg) significantly reduced the myocardial infarct size after I/R, while dmCAPA (15 mg/kg) had no cardioprotective effect. Interestingly, pretreatment with a NOS inhibitor, (L-NAME, 3 mg/kg) eliminated the effect of CAPA on myocardial infarction. Additionally, a 4-week CAPA treatment (1 mg/kg, orally, once daily) started 4 weeks after STZ-induction could effectively decrease the infarct size and ameliorate the cardiac dysfunction by pressure-volume loop analysis in STZ-induced diabetic animals.
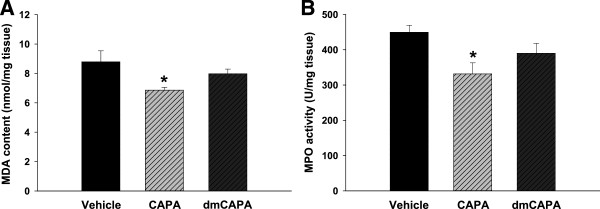
Conclusions: CAPA, which is structurally similar to CAPE, exerts cardioprotective activity in I/R injury through its antioxidant property and by preserving nitric oxide levels. On the other hand, chronic CAPA treatment could also ameliorate cardiac dysfunction in diabetic animals.
Figures
References
-
- Di Filippo C, Marfella R, Cuzzocrea S, Piegari E, Petronella P, Giugliano D, Rossi F, D'Amico M. Hyperglycemia in streptozotocin-induced diabetic rat increases infarct size associated with low levels of myocardial HO-1 during ischemia/reperfusion. Diabetes. 2005;54:803–810. doi: 10.2337/diabetes.54.3.803. - DOI - PubMed
-
- Marfella R, D'Amico M, Di Filippo C, Piegari E, Nappo F, Esposito K, Berrino L, Rossi F, Giugliano D. Myocardial infarction in diabetic rats: role of hyperglycaemia on infarct size and early expression of hypoxia-inducible factor 1. Diabetologia. 2002;45:1172–1181. doi: 10.1007/s00125-002-0882-x. - DOI - PubMed
-
- Simpson PJ, Lucchesi BR. Free radicals and myocardial ischemia and reperfusion injury. J Lab Clin Med. 1987;110:13–30. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
