

Success or failure of critical steps in community case management of malaria with rapid diagnostic tests: a systematic review
- PMID: 24924295
- PMCID: PMC4084582
- DOI: 10.1186/1475-2875-13-229
Success or failure of critical steps in community case management of malaria with rapid diagnostic tests: a systematic review
Abstract
Background: Malaria still causes high morbidity and mortality around the world, mainly in sub-Saharan Africa. Community case management of malaria (CCMm) by community health workers (CHWs) is one of the strategies to combat the disease by increasing access to malaria treatment. Currently, the World Health Organization recommends to treat only confirmed malaria cases, rather than to give presumptive treatment.
Objectives: This systematic review aims to provide a comprehensive overview of the success or failure of critical steps in CCMm with rapid diagnostic tests (RDTs).
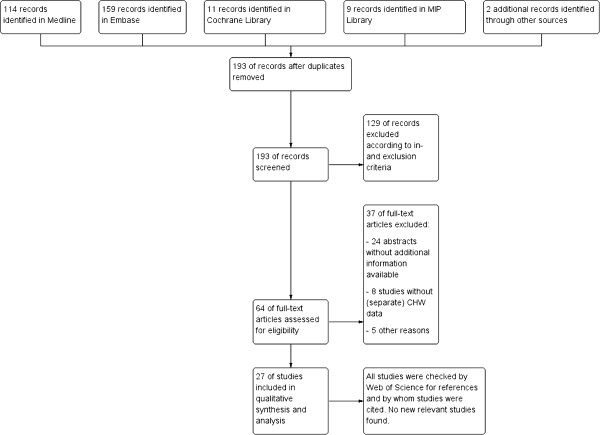
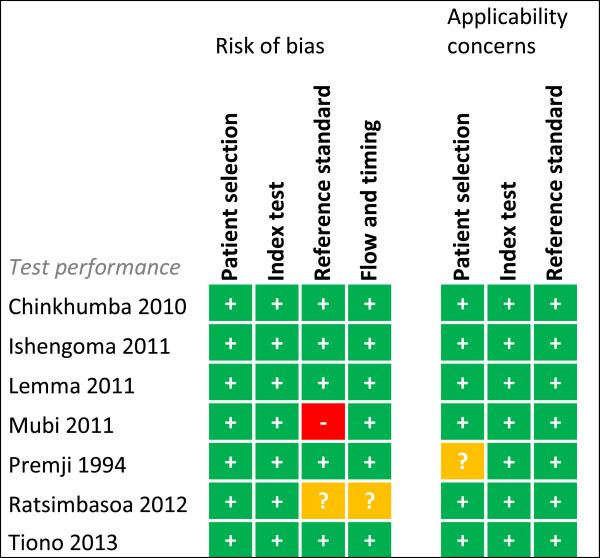
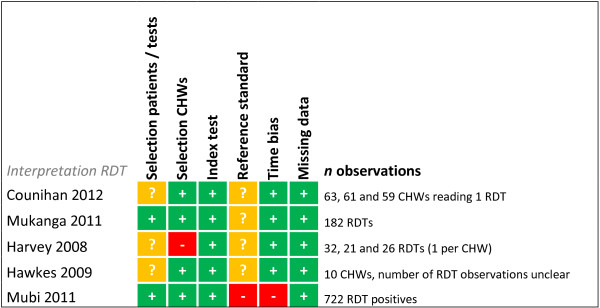
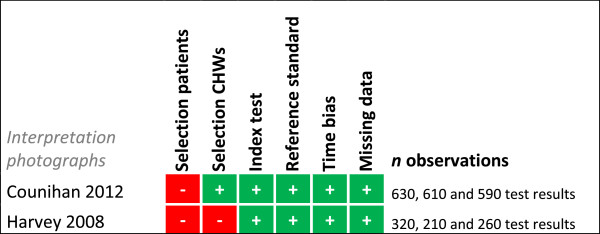
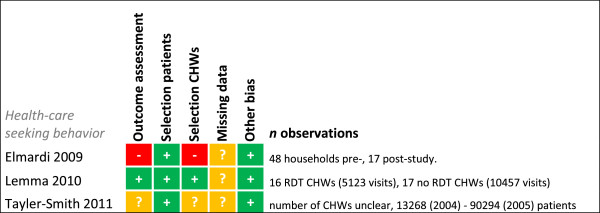
Methods: The databases of Medline, Embase, the Cochrane Library, the library of the 'Malaria in Pregnancy' consortium, and Web of Science were used to find studies on CCMm with RDTs in SSA. Studies were selected according to inclusion and exclusion criteria, subsequently risk of bias was assessed and data extracted.
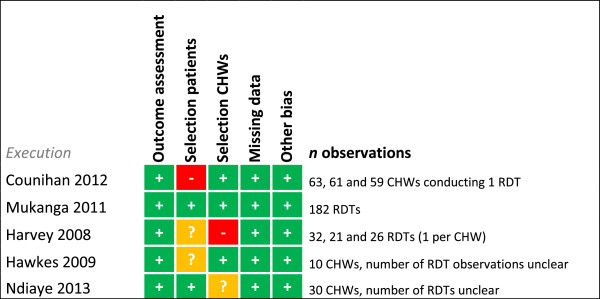
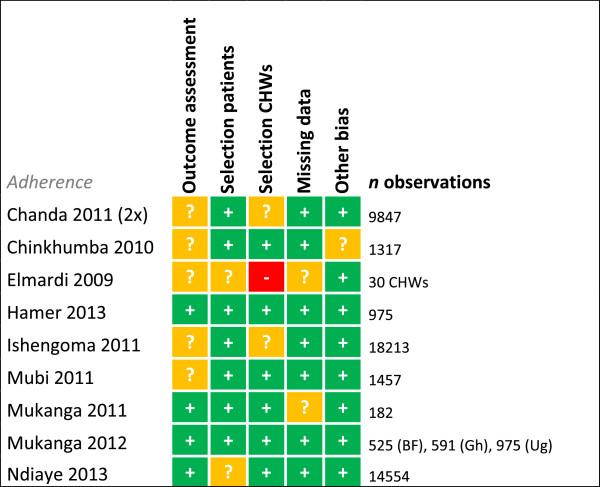
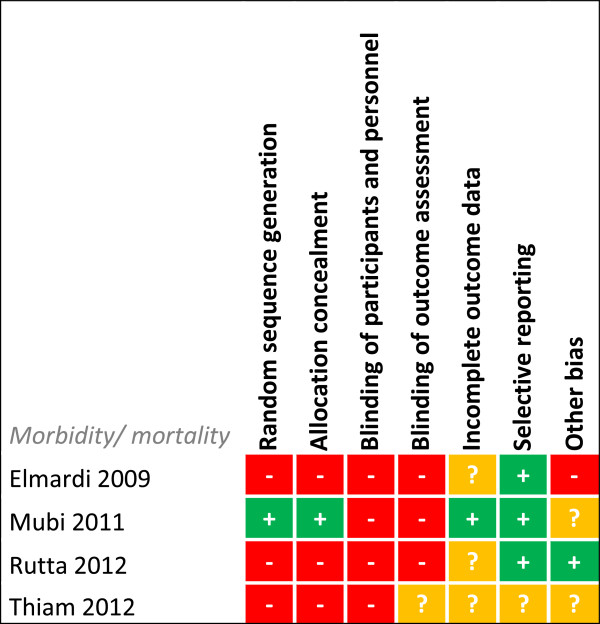
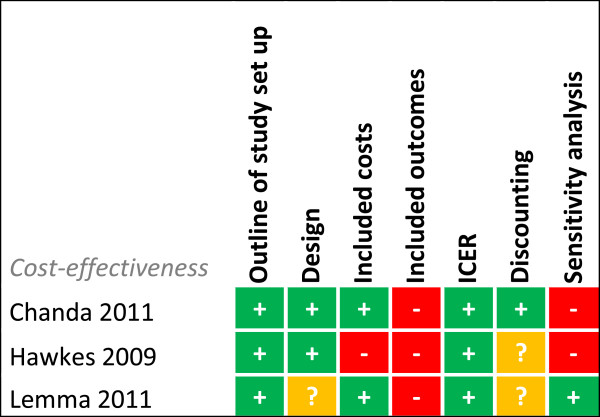
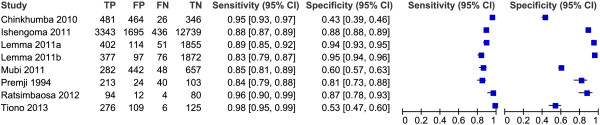
Results: 27 articles were included. CHWs were able to correctly perform RDTs, although specificity levels were variable. CHWs showed high adherence to test results, but in some studies a substantial group of RDT negatives received treatment. High risk of bias was found for morbidity and mortality studies, therefore, effects on morbidity and mortality could not be estimated. Uptake and acceptance by the community was high, however negative-tested patients did not always follow up referral advice. Drug or RDT stock-outs and limited information on CHW motivation are bottlenecks for sustainable implementation. RDT-based CCMm was found to be cost effective for the correct treatment of malaria in areas with low to medium malaria prevalence, but study designs were not optimal.
Discussion: Trained CHWs can deliver high quality care for malaria using RDTs. However, lower RDT specificity could lead to missed diagnoses of non-malarial causes of fever. Other threats for CCMm are non-adherence to negative test results and low referral completion. Integrated CCM may solve some of these issues. Unfortunately, morbidity and mortality are not adequately investigated. More information is needed about influencing sociocultural aspects, CHW motivation and stock supply.
Conclusion: CCMm is generally well executed by CHWs, but there are several barriers for its success. Integrated CCM may overcome some of these barriers.
Figures
References
-
- Sachs J, Malaney P. The economic and social burden of malaria. Nature. 2002;415:680–685. - PubMed
-
- World Health Organization. The Roll Back Malaria Strategy for Improving Access to Treatment through Home Management of Malaria. Geneva: World Health Organization; 2005. pp. 1–52.
-
- World Health Organization. Guidelines for the Treatment of Malaria. Geneva: World Health Organization; 2010. pp. 1–194.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
