

Comparative definitions for moderate-severe ischemia in stress nuclear, echocardiography, and magnetic resonance imaging
- PMID: 24925328
- PMCID: PMC4128344
- DOI: 10.1016/j.jcmg.2013.10.021
Comparative definitions for moderate-severe ischemia in stress nuclear, echocardiography, and magnetic resonance imaging
Erratum in
- JACC Cardiovasc Imaging. 2014 Jul;7(7):748
Abstract
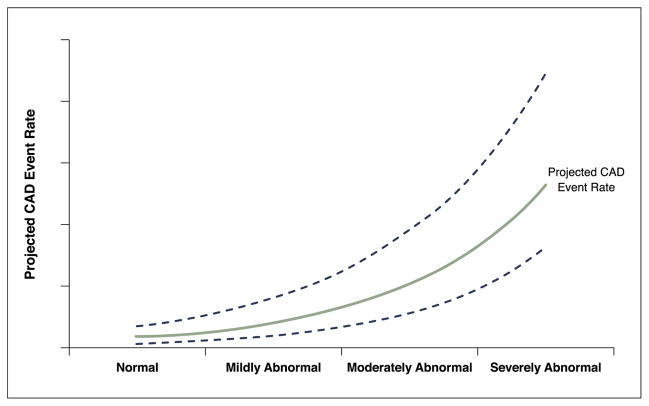
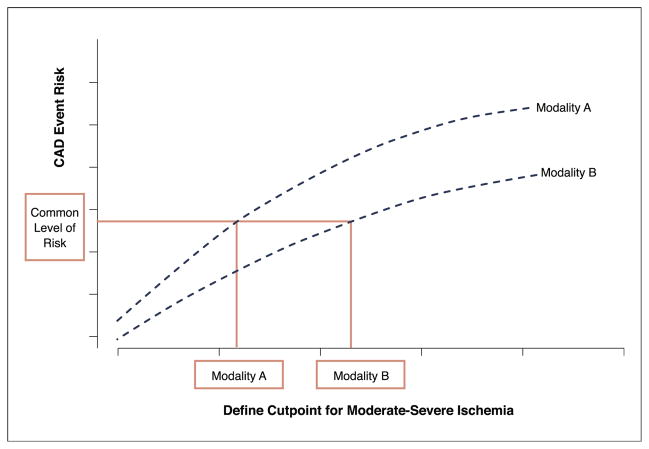
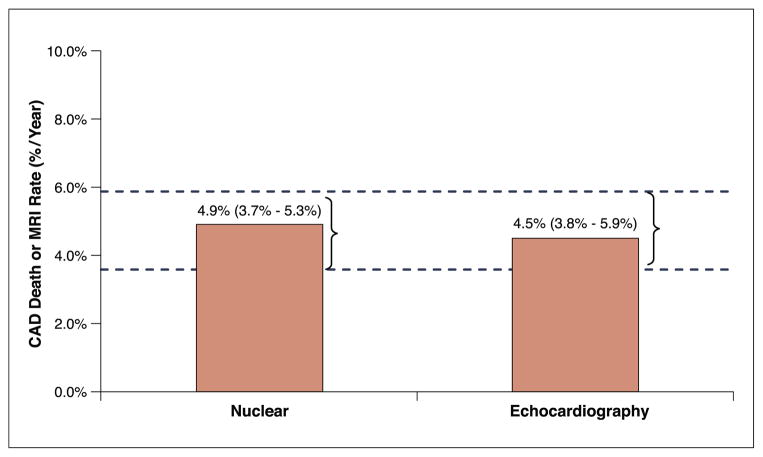
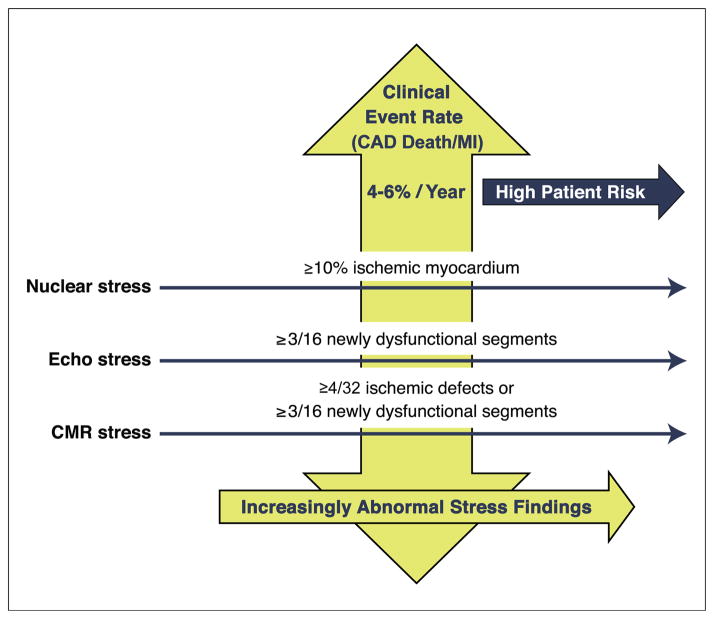
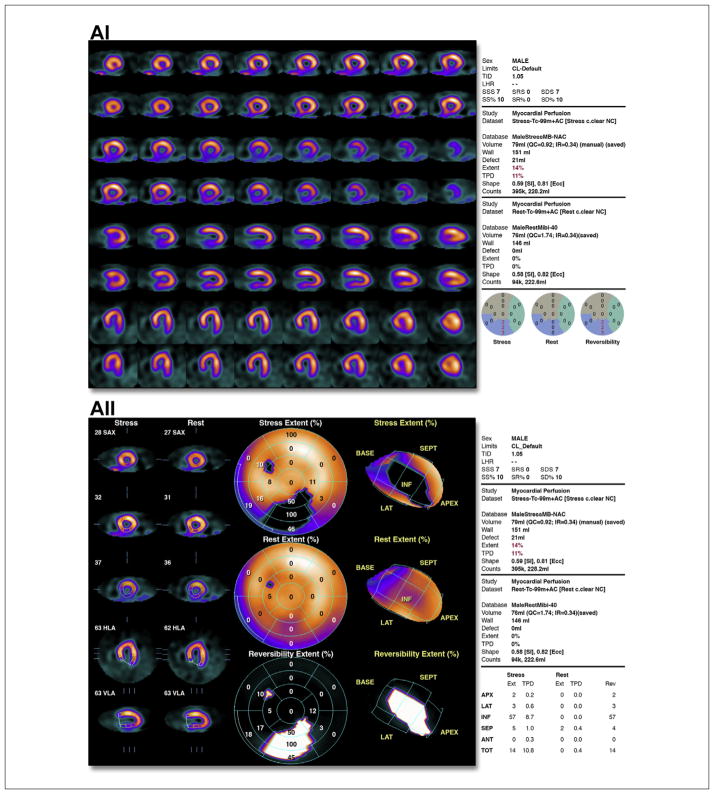
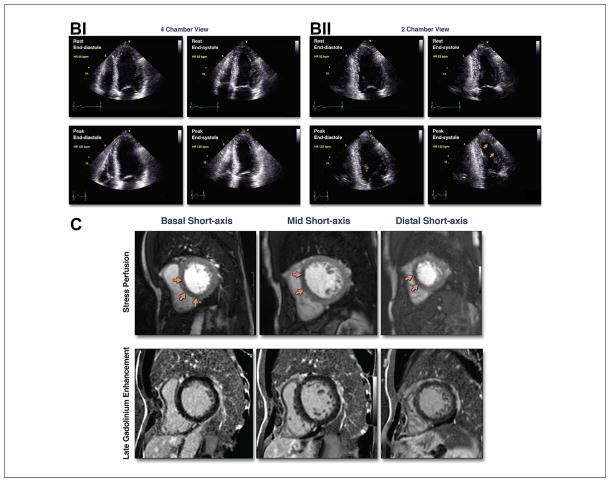
The lack of standardized reporting of the magnitude of ischemia on noninvasive imaging contributes to variability in translating the severity of ischemia across stress imaging modalities. We identified the risk of coronary artery disease (CAD) death or myocardial infarction (MI) associated with ≥10% ischemic myocardium on stress nuclear imaging as the risk threshold for stress echocardiography and cardiac magnetic resonance. A narrative review revealed that ≥10% ischemic myocardium on stress nuclear imaging was associated with a median rate of CAD death or MI of 4.9%/year (interquartile range: 3.75% to 5.3%). For stress echocardiography, ≥3 newly dysfunctional segments portend a median rate of CAD death or MI of 4.5%/year (interquartile range: 3.8% to 5.9%). Although imprecisely delineated, moderate-severe ischemia on cardiac magnetic resonance may be indicated by ≥4 of 32 stress perfusion defects or ≥3 dobutamine-induced dysfunctional segments. Risk-based thresholds can define equivalent amounts of ischemia across the stress imaging modalities, which will help to translate a common understanding of patient risk on which to guide subsequent management decisions.
Keywords: cardiac imaging; ischemia; prognosis.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease. J Am Coll Cardiol. 2012;60:e44–164. - PubMed
-
- Hendel RC, Berman DS, Di Carli MF, et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging. J Am Coll Cardiol. 2009;53:2201–29. - PubMed
-
- Douglas PS, Khandheria B, Stainback RF, et al. ACCF/ASE/ACEP/AHA/ASNC/SCAI/SCCT/SCMR 2008 appropriateness criteria for stress echocardiography. J Am Coll Cardiol. 2008;51:1127–47. - PubMed
-
- Shaw LJ, Shaw RE, Merz CN, et al. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and inhospital mortality in the american college of cardiology-national cardiovascular data registry. Circulation. 2008;117:1787–801. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
