

A versatile model of open-fracture infection : a contaminated segmental rat femur defect
- PMID: 24926038
- PMCID: PMC4054011
- DOI: 10.1302/2046-3758.36.2000293
A versatile model of open-fracture infection : a contaminated segmental rat femur defect
Abstract
Objectives: The purpose of this study was to refine an accepted contaminated rat femur defect model to result in an infection rate of approximately 50%. This threshold will allow examination of treatments aimed at reducing infection in open fractures with less risk of type II error.
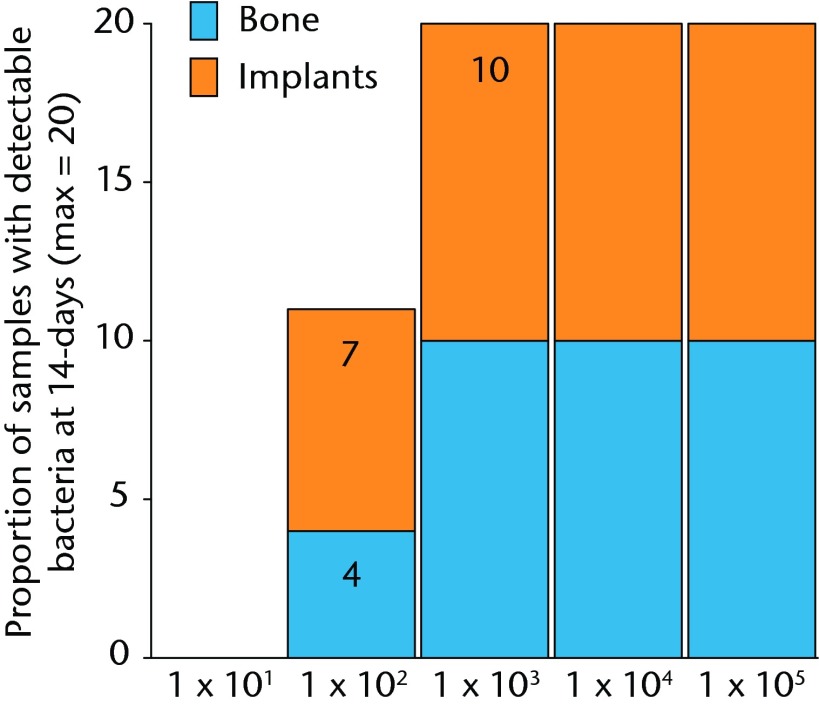
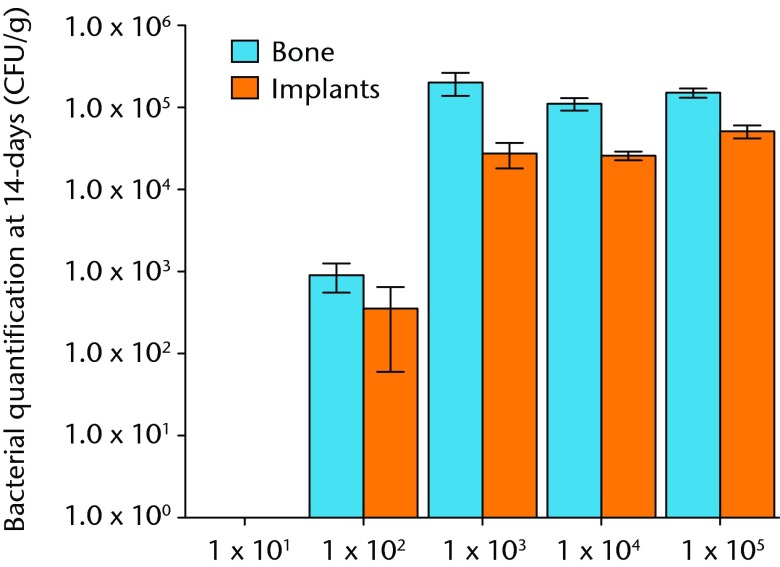
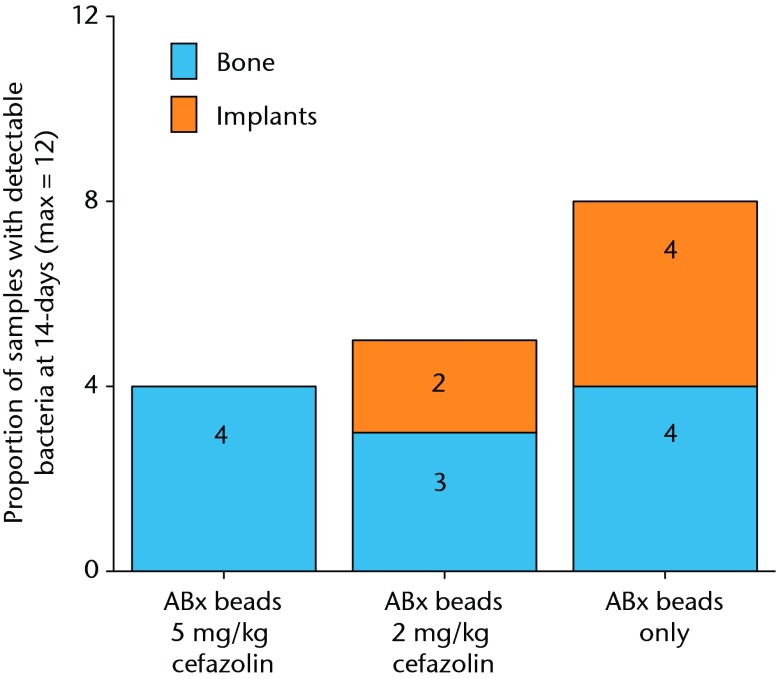
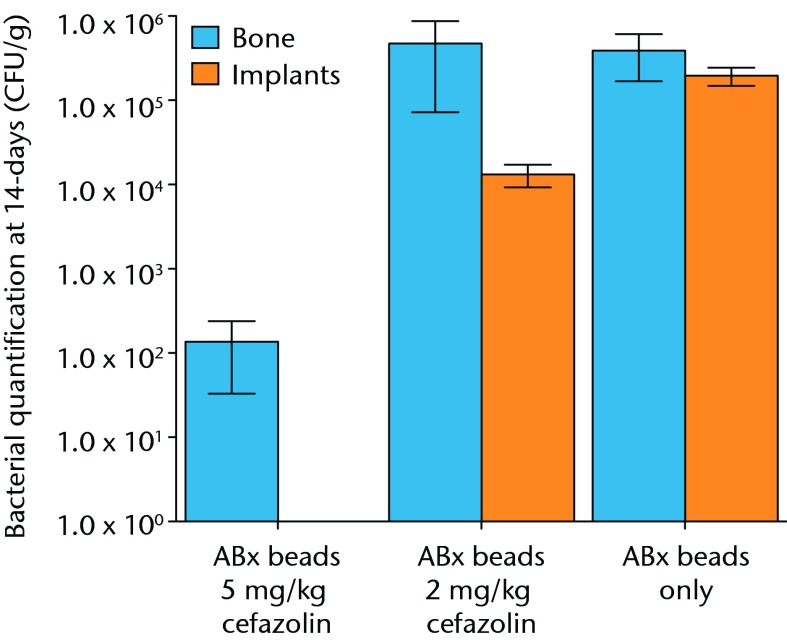
Methods: Defects were created in the stablised femurs of anaethetised rats, contaminated with Staphylococcus aureus and then debrided and irrigated six hours later. After 14 days, the bone and implants were harvested for separate microbiological analysis. This basic model was developed in several studies by varying the quantity of bacterial inoculation, introducing various doses of systemic antibiotics with and without local antibiotics.
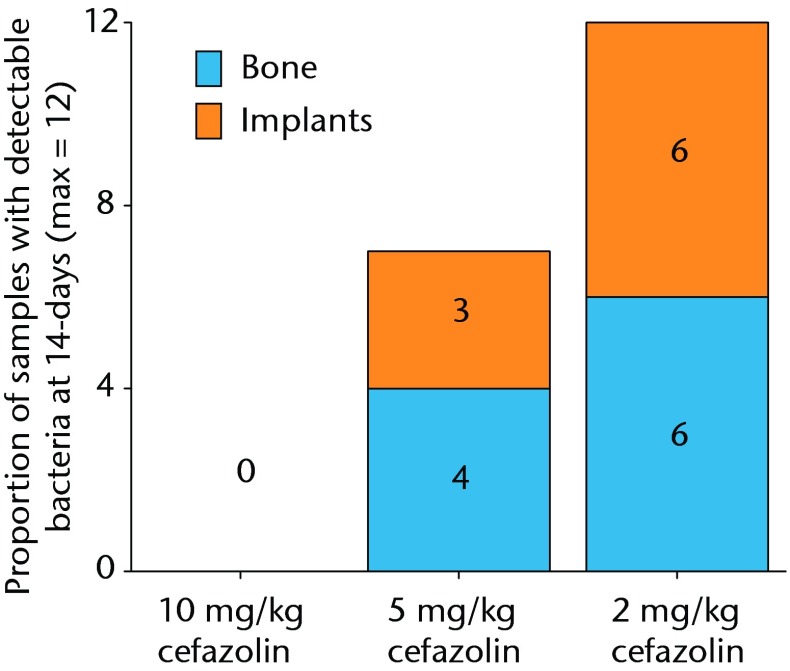
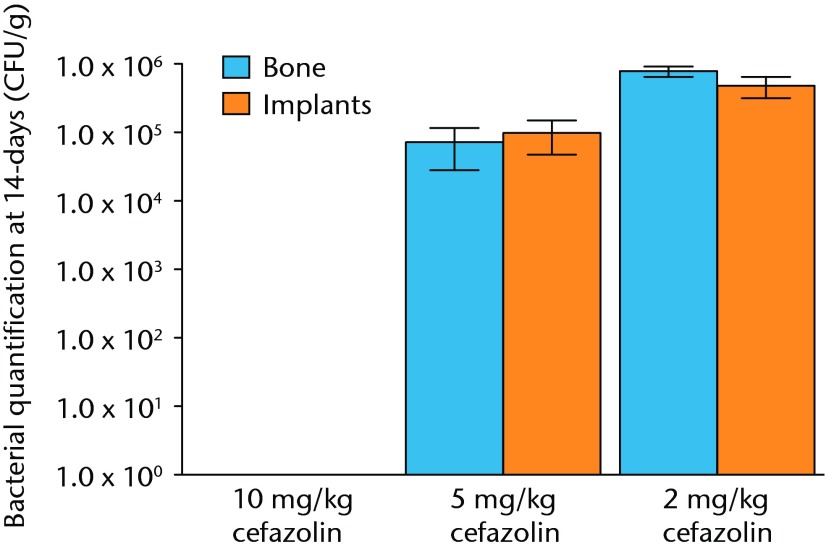
Results: The bacterial inoculation associated with a 50% infection rate was established as 1 × 10(2) colony forming units (CFU). With an initial bacterial inoculum of 1 × 10(5) CFU, the dose of systemic antibiotics associated with 50% infection was 5 mg/Kg of cafazolin injected sub-cutaneously every 12 hours, starting at the time of the first debridment and continuing for 72 hours (seven doses). The systemic dose of cafazolin was lowered to 2 mg/Kg when antibiotic polymethyl methacrylate beads were used concurrently with the same amount of bacterial inoculation.
Conclusion: This model of open fracture infection has been further refined with potential for local and systemic antibiotics. This is a versatile model and with the concepts presented herein, it can be modified to evaluate various emerging therapies and concepts for open fractures. Cite this article: Bone Joint Res 2014;3:187-92.
Keywords: Infection; Open fracture; Contamination; Animal-model; Local antibiotics.
©2014 The British Editorial Society of Bone & Joint Surgery.
Conflict of interest statement
Figures

References
-
- MacKenzie EJ, Bosse MJ, Pollak AN, et al. Long-term persistence of disability following severe lower-limb trauma. Results of a seven-year follow-up. J Bone Joint Surg [Am] 2005;87-A:1801–1809 - PubMed
-
- Penn-Barwell JG, Bennett PM, Fries CA, et al. Severe open tibial fractures in combat trauma: management and preliminary outcomes. Bone Joint J 2013;95-B:101–105 - PubMed
-
- Anglen JO. Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds. A prospective, randomized study. J Bone Joint Surg [Am] 2005;87-A:1415–1422 - PubMed
-
- Chen X, Kidder LS, Lew WD. Osteogenic protein-1 induced bone formation in an infected segmental defect in the rat femur. J Orthop Res 2002;20:142–150 - PubMed
-
- Petty W, Spanier S, Shuster JJ, Silverthorne C. The influence of skeletal implants on incidence of infection. Experiments in a canine model. J Bone Joint Surg [Am] 1985;67-A:1236–1244 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
