

The bilirubin albumin ratio in the management of hyperbilirubinemia in preterm infants to improve neurodevelopmental outcome: a randomized controlled trial--BARTrial
- PMID: 24927259
- PMCID: PMC4057208
- DOI: 10.1371/journal.pone.0099466
The bilirubin albumin ratio in the management of hyperbilirubinemia in preterm infants to improve neurodevelopmental outcome: a randomized controlled trial--BARTrial
Abstract
Background and objective: High bilirubin/albumin (B/A) ratios increase the risk of bilirubin neurotoxicity. The B/A ratio may be a valuable measure, in addition to the total serum bilirubin (TSB), in the management of hyperbilirubinemia. We aimed to assess whether the additional use of B/A ratios in the management of hyperbilirubinemia in preterm infants improved neurodevelopmental outcome.
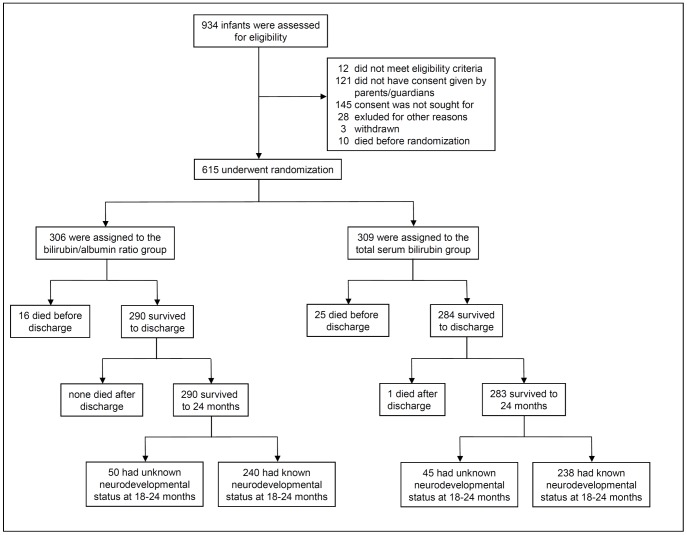
Methods: In a prospective, randomized controlled trial, 615 preterm infants of 32 weeks' gestation or less were randomly assigned to treatment based on either B/A ratio and TSB thresholds (consensus-based), whichever threshold was crossed first, or on the TSB thresholds only. The primary outcome was neurodevelopment at 18 to 24 months' corrected age as assessed with the Bayley Scales of Infant Development III by investigators unaware of treatment allocation. Secondary outcomes included complications of preterm birth and death.
Results: Composite motor (100 ± 13 vs. 101 ± 12) and cognitive (101 ± 12 vs. 101 ± 11) scores did not differ between the B/A ratio and TSB groups. Demographic characteristics, maximal TSB levels, B/A ratios, and other secondary outcomes were similar. The rates of death and/or severe neurodevelopmental impairment for the B/A ratio versus TSB groups were 15.4% versus 15.5% (P = 1.0) and 2.8% versus 1.4% (P = 0.62) for birth weights ≤ 1000 g and 1.8% versus 5.8% (P = 0.03) and 4.1% versus 2.0% (P = 0.26) for birth weights of >1000 g.
Conclusions: The additional use of B/A ratio in the management of hyperbilirubinemia in preterm infants did not improve their neurodevelopmental outcome.
Trial registration: Controlled-Trials.com ISRCTN74465643.
Conflict of interest statement
Figures
References
-
- Wennberg RP, Ahlfors CE, Bhutani VK, Johnson LH, Shapiro SM (2006) Toward understanding kernicterus: A challenge to improve the management of jaundiced newborns. Pediatrics 117: 474–485. - PubMed
-
- McDonagh A, Maisels MJ (2006) Bilirubin unbound: Deja vu all over again? Pediatrics 117: 523–525. - PubMed
-
- Ahlfors CE (2010) Predicting bilirubin neurotoxicity in jaundiced newborns. Curr Opin Pediatr 22: 129–133. - PubMed
-
- Watchko JF, Tiribelli C (2013) Bilirubin-induced neurologic damage–mechanisms and management approaches. N Engl J Med 369: 2021–2030. - PubMed
-
- Hulzebos CV, van Imhoff DE, Bos AF, Ahlfors CE, Verkade HJ, et al. (2008) Usefulness of the bilirubin/albumin ratio for predicting bilirubin-induced neurotoxicity in premature infants. Arch Dis Child Fetal Neonatal Ed 93: F384–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
