

Idiopathic pulmonary fibrosis: CT and risk of death
- PMID: 24927326
- PMCID: PMC4334234
- DOI: 10.1148/radiol.14130216
Idiopathic pulmonary fibrosis: CT and risk of death
Abstract
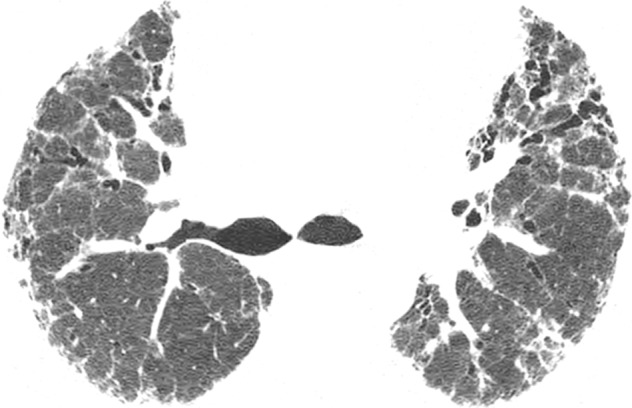
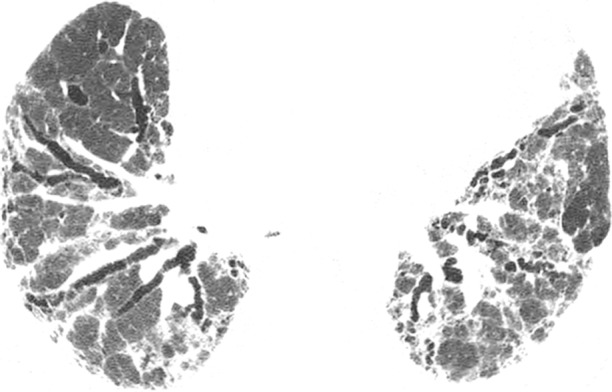
Purpose: To investigate the prognostic value of quantitative computed tomographic (CT) scoring for the extent of fibrosis or emphysema in the context of a clinical model that includes the gender, age, and physiology ( GAP gender, age, and physiology model) of the patient.
Materials and methods: Study cohorts were approved by local institutional review boards, and all patients provided written consent. This was a retrospective cohort study that included 348 patients (246 men, 102 women; mean age, 69 years ± 9) with idiopathic pulmonary fibrosis from two institutions. Fibrosis and emphysema visual scores were independently determined by two radiologists. Models were based on competing risks regression for death and were evaluated by using the C index and reclassification improvement.
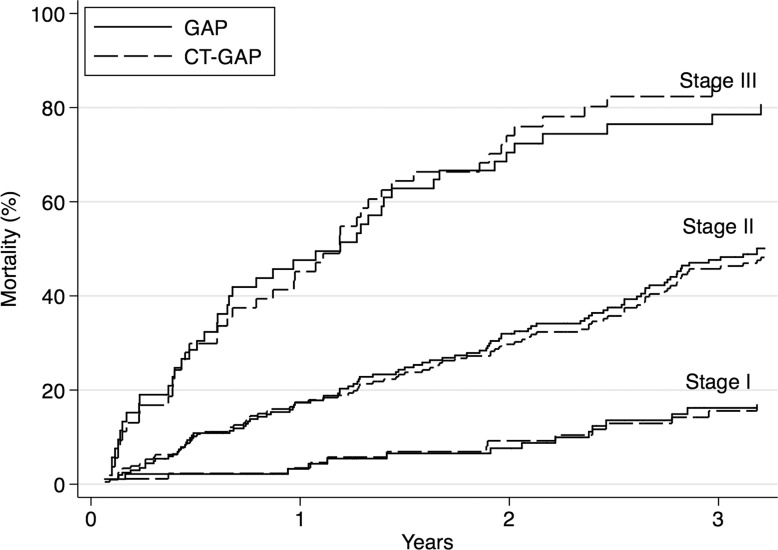
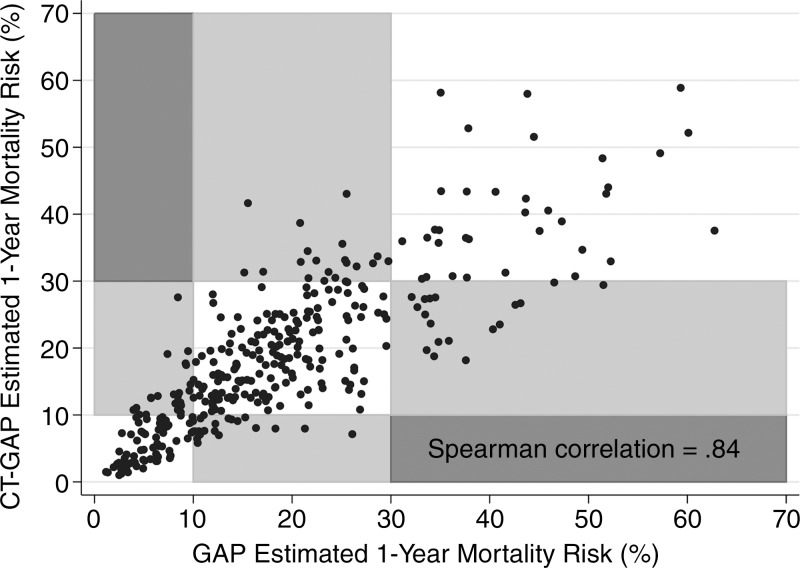
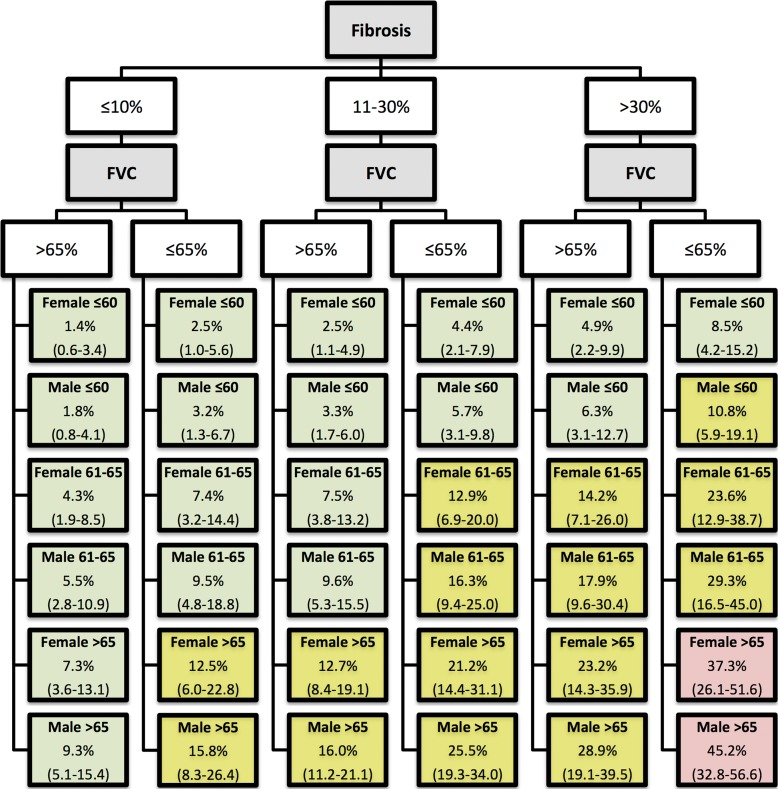
Results: The CT- GAP gender, age, and physiology model (a modification of the original GAP gender, age, and physiology model that replaces diffusion capacity of carbon monoxide with CT fibrosis score) had accuracy comparable to that of the original GAP gender, age, and physiology model, with a C index of 70.3 (95% confidence interval: 66.4, 74.0); difference in C index compared with the GAP gender, age, and physiology model of -0.4 (95% confidence interval: -2.2, 3.4). The performance of the original GAP gender, age, and physiology model did not change significantly with the simple addition of fibrosis score, with a change in C index of 0.0 (95% confidence interval: -1.8, 0.5) or of emphysema score, with a change in C index of 0.0 [95% confidence interval: -1.3, 0.4]).
Conclusion: CT fibrosis score can replace diffusion capacity of carbon monoxide test results in a modified GAP gender, age, and physiology model (the CT- GAP gender, age, and physiology model) with comparable performance. This may be a useful alternative model in situations where CT scoring is more reliable and available than diffusion capacity of carbon monoxide.
Figures



References
-
- Martinez FJ, Safrin S, Weycker D, et al. ; IPF Study Group . The clinical course of patients with idiopathic pulmonary fibrosis. Ann Intern Med 2005;142(12 Pt 1):963–967. - PubMed
-
- King TE, Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: scoring system and survival model. Am J Respir Crit Care Med 2001;164(7):1171–1181. - PubMed
-
- Wells AU, Desai SR, Rubens MB, et al. Idiopathic pulmonary fibrosis: a composite physiologic index derived from disease extent observed by computed tomography. Am J Respir Crit Care Med 2003;167(7):962–969. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
