

Comparison of spatially matched airways reveals thinner airway walls in COPD. The Multi-Ethnic Study of Atherosclerosis (MESA) COPD Study and the Subpopulations and Intermediate Outcomes in COPD Study (SPIROMICS)
- PMID: 24928812
- PMCID: PMC4198462
- DOI: 10.1136/thoraxjnl-2014-205160
Comparison of spatially matched airways reveals thinner airway walls in COPD. The Multi-Ethnic Study of Atherosclerosis (MESA) COPD Study and the Subpopulations and Intermediate Outcomes in COPD Study (SPIROMICS)
Abstract
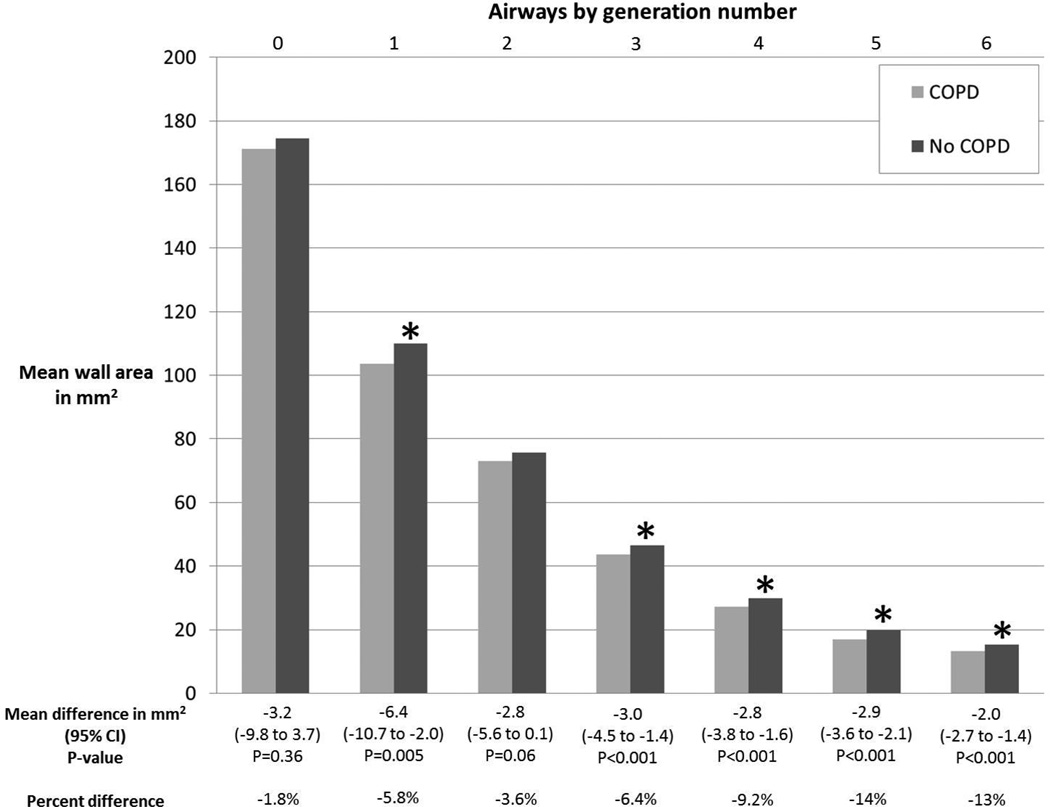
Background: COPD is characterised by reduced airway lumen dimensions and fewer peripheral airways. Most studies of airway properties sample airways based upon lumen dimension or at random, which may bias comparisons given reduced airway lumen dimensions and number in COPD. We sought to compare central airway wall dimensions on CT in COPD and controls using spatially matched airways, thereby avoiding selection bias of airways in the lung.
Methods: The Multi-Ethnic Study of Atherosclerosis (MESA) COPD Study and Subpopulations and Intermediate Outcomes in COPD Study (SPIROMICS) recruited smokers with COPD and controls aged 50-79 years and 40-80 years, respectively. COPD was defined by current guidelines. Using CT image data, airway dimensions were measured for all central airway segments (generations 0-6) following 5 standardised paths into the lungs. Case-control airway comparisons were spatially matched by generation and adjusted for demographics, body size, smoking, CT dose, per cent emphysema, airway length and lung volume.
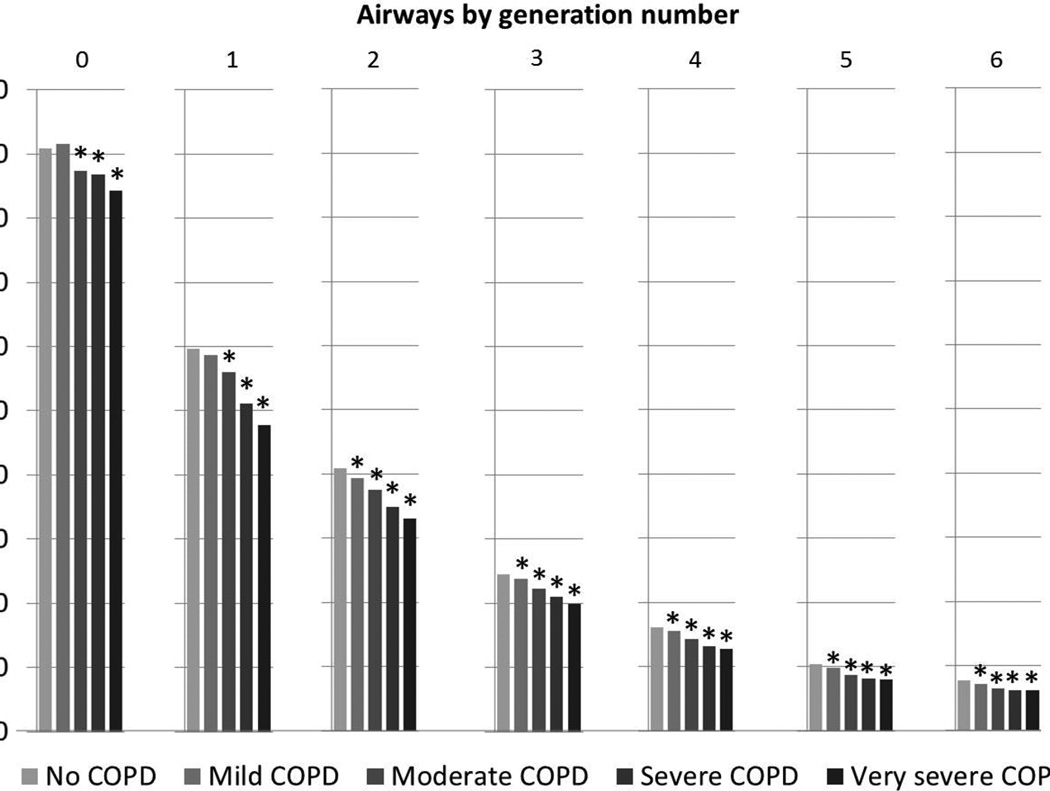
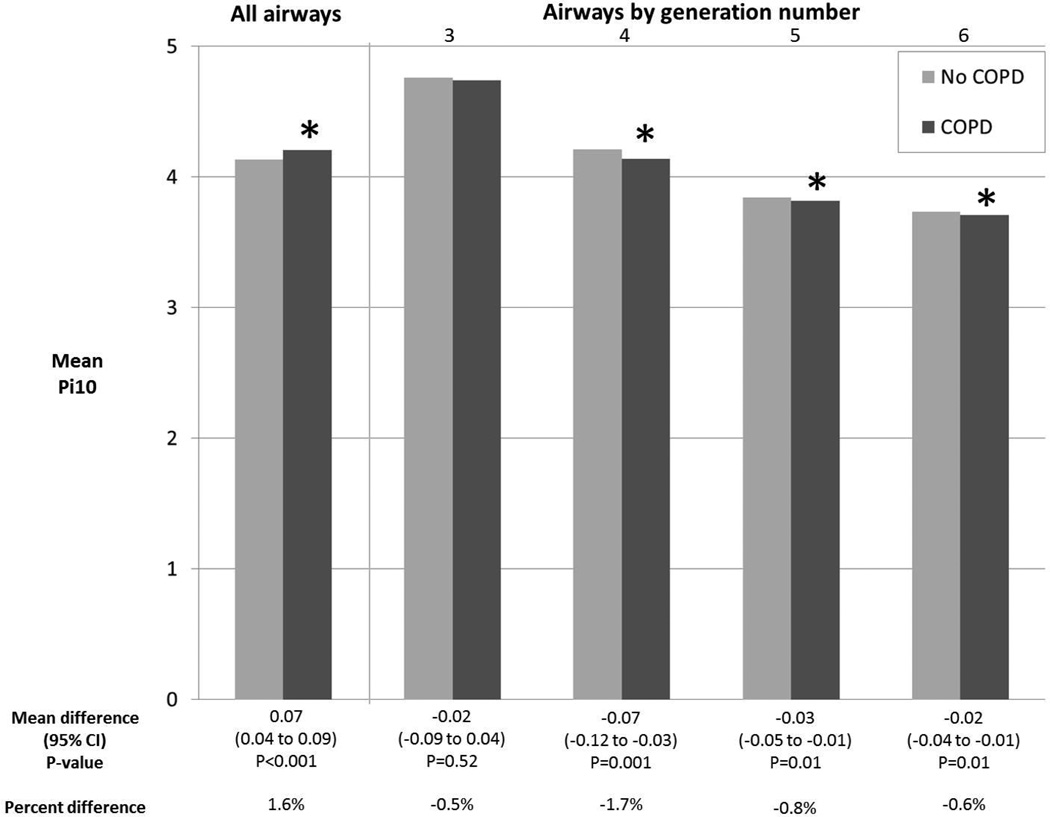
Results: Among 311 MESA COPD participants, airway wall areas at generations 3-6 were smaller in COPD compared with controls (all p<0.001). Among 1248 SPIROMICS participants, airway wall areas at generations 1-6 were smaller (all p<0.001), and this reduction was monotonic with increasing COPD severity (p<0.001). In both studies, sampling airways by lumen diameter or randomly resulted in a comparison of more proximal airways in COPD to more peripheral airways in controls (p<0.001) resulting in the appearance of thicker walls in COPD (p<0.02).
Conclusions: Airway walls are thinner in COPD when comparing spatially matched central airways. Other approaches to airway sampling result in comparisons of more proximal to more distal airways and potentially biased assessment of airway properties in COPD.
Keywords: COPD epidemiology; Imaging/CT MRI etc.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Figures
Comment in
-
Is the 'spatially matched central airways' relevant to studies of airway dimensions in COPD?Thorax. 2014 Nov;69(11):1048-9. doi: 10.1136/thoraxjnl-2014-206118. Epub 2014 Sep 5. Thorax. 2014. PMID: 25192710 No abstract available.
-
Airway anatomy as a risk factor of COPD.Thorax. 2015 Jun;70(6):586. doi: 10.1136/thoraxjnl-2014-206534. Epub 2014 Dec 8. Thorax. 2015. PMID: 25487571 No abstract available.
-
Author's response: Airway anatomy in COPD: many dimensions to consider.Thorax. 2015 Jun;70(6):585. doi: 10.1136/thoraxjnl-2014-206606. Epub 2015 Jan 8. Thorax. 2015. PMID: 25572599 No abstract available.
References
-
- Vestbo J, Hurd SS, Agusti AG, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease GOLD Executive Summary. American journal of respiratory and critical care medicine. 2013;187(4):347–365. - PubMed
-
- Fishman AP, Macklem PT, Mead J, et al. Handbook of physiology. 2v. Bethesda, Md: American Physiological Society; 1986. Mechanics of breathing; p. xxv, 784.
-
- Weibel ER. Morphometry of the human lung. Berlin: Springer; 1963.
-
- Tiddens HA, Pare PD, Hogg JC, et al. Cartilaginous airway dimensions and airflow obstruction in human lungs. American journal of respiratory and critical care medicine. 1995;152(1):260–266. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases