

Improving inhaler adherence in patients with chronic obstructive pulmonary disease: a cost-effectiveness analysis
- PMID: 24929799
- PMCID: PMC4067522
- DOI: 10.1186/1465-9921-15-66
Improving inhaler adherence in patients with chronic obstructive pulmonary disease: a cost-effectiveness analysis
Abstract
Background: The PHARMACOP-intervention significantly improved medication adherence and inhalation technique for patients with COPD compared with usual care. This study aimed to evaluate its cost-effectiveness.
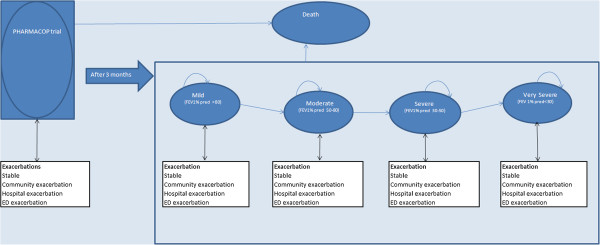
Methods: An economic analysis was performed from the Belgian healthcare payer's perspective. A Markov model was constructed in which a representative group of patients with COPD (mean age of 70 years, 66% male, 43% current smokers and mean Forced Expiratory Volume in 1 second of % predicted of 50), was followed for either receiving the 3-month PHARMACOP-intervention or usual care. Three types of costs were calculated: intervention costs, medication costs and exacerbation costs. Outcome measures included the number of hospital-treated exacerbations, cost per prevented hospital-treated exacerbation and cost per Quality Adjusted Life-Year. Follow-up was 1 year in the basecase analysis. Sensitivity and scenario analyses (including long-term follow-up) were performed to assess uncertainty.
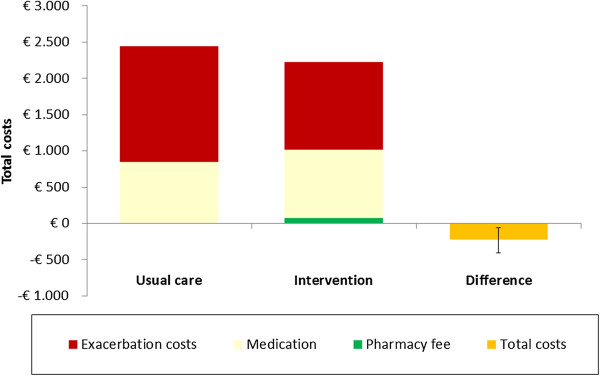
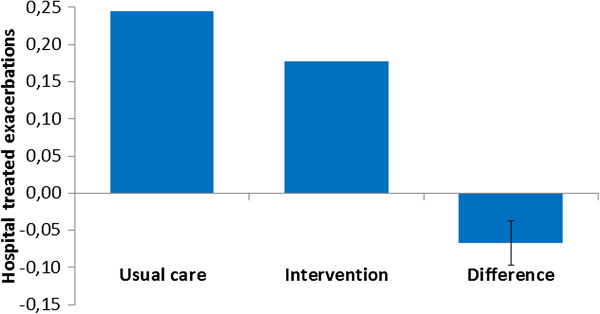
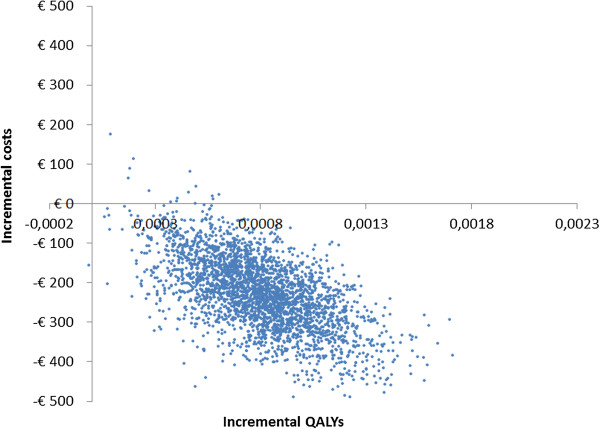
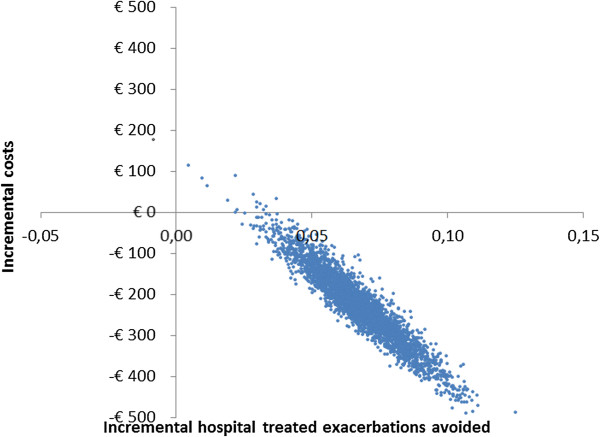
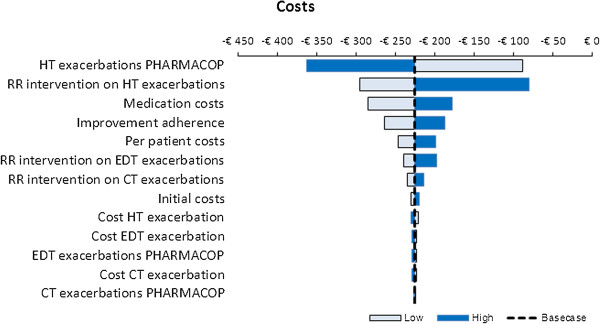
Results: In the basecase analysis, the average overall costs per patient for the PHARMACOP-intervention and usual care were €2,221 and €2,448, respectively within the 1-year time horizon. This reflects cost savings of €227 for the PHARMACOP-intervention. The PHARMACOP-intervention resulted in the prevention of 0.07 hospital-treated exacerbations per patient (0.177 for PHARMACOP versus 0.244 for usual care). Results showed robust cost-savings in various sensitivity analyses.
Conclusions: Optimization of current pharmacotherapy (e.g. close monitoring of inhalation technique and medication adherence) has been shown to be cost-saving and should be considered before adding new therapies.
Figures
References
-
- World Health Organization. Chronic obstructive pulmonary disease. http://www.who.int/respiratory/copd/en.
-
- Scientific Institute for Public Health Belgium (WIV-ISP) https://www.wiv-isp.be.
-
- From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2013. http://www.goldcopd.org.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
