

Cell-surface central nervous system autoantibodies: clinical relevance and emerging paradigms
- PMID: 24930434
- PMCID: PMC4141019
- DOI: 10.1002/ana.24200
Cell-surface central nervous system autoantibodies: clinical relevance and emerging paradigms
Abstract
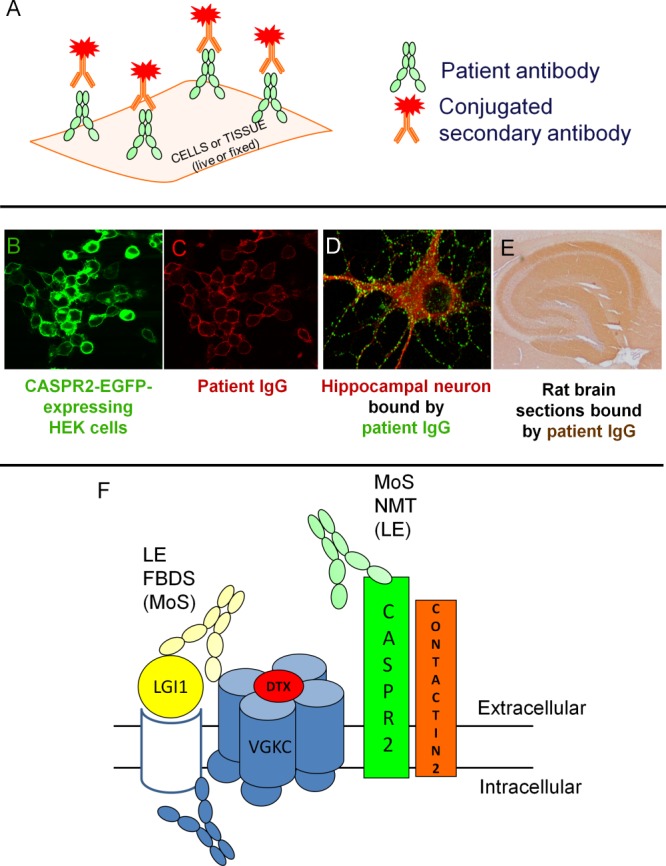
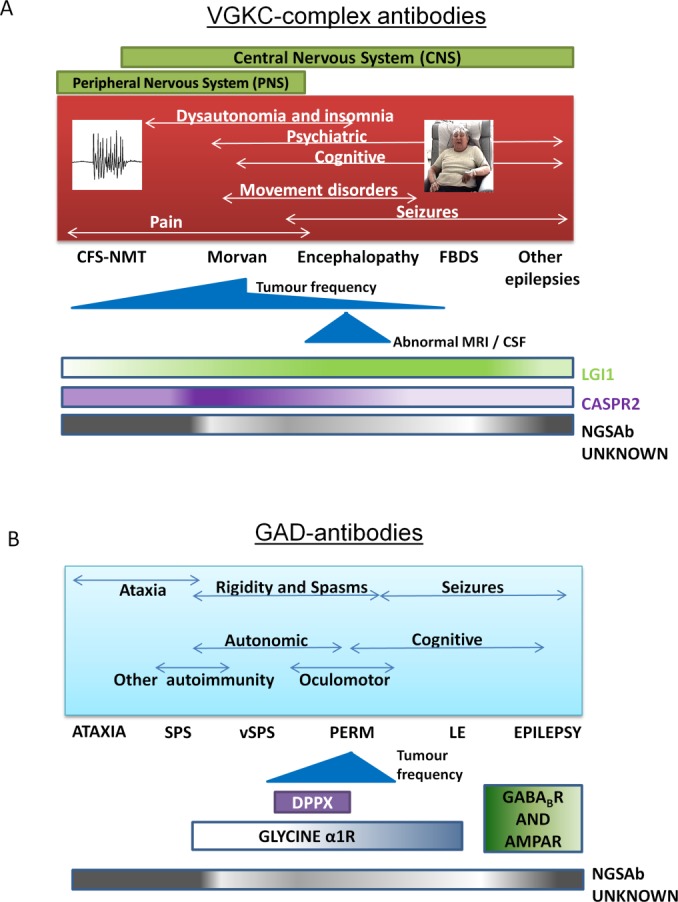
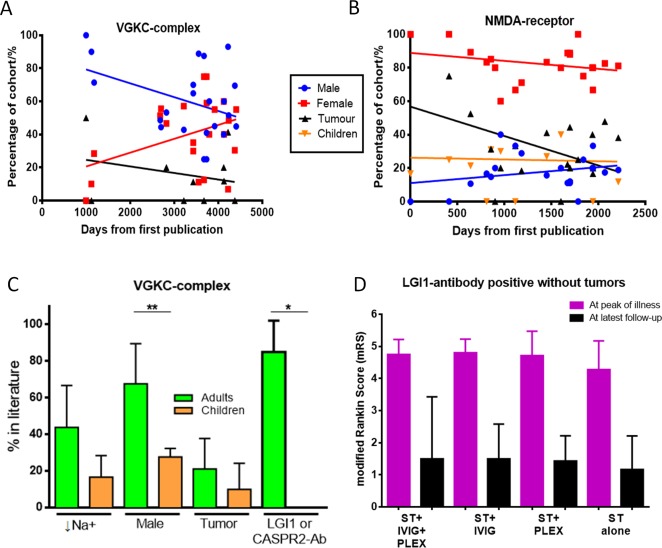
The recent discovery of several potentially pathogenic autoantibodies has helped identify patients with clinically distinctive central nervous system diseases that appear to benefit from immunotherapy. The associated autoantibodies are directed against the extracellular domains of cell-surface-expressed neuronal or glial proteins such as LGI1, N-methyl-D-aspartate receptor, and aquaporin-4. The original descriptions of the associated clinical syndromes were phenotypically well circumscribed. However, as availability of antibody testing has increased, the range of associated patient phenotypes and demographics has expanded. This in turn has led to the recognition of more immunotherapy-responsive syndromes in patients presenting with cognitive and behavioral problems, seizures, movement disorders, psychiatric features, and demyelinating disease. Although antibody detection remains diagnostically important, clinical recognition of these distinctive syndromes should ensure early and appropriate immunotherapy administration. We review the emerging paradigm of cell-surface-directed antibody-mediated neurological diseases, describe how the associated disease spectrums have broadened since the original descriptions, discuss some of the methodological issues regarding techniques for antibody detection and emphasize considerations surrounding immunotherapy administration. As these disorders continue to reach mainstream neurology and even psychiatry, more cell-surface-directed antibodies will be discovered, and their possible relevance to other more common disease presentations should become more clearly defined.
© 2014 American Neurological Association.
Figures
References
-
- McKeon A, Pittock SJ. Paraneoplastic encephalomyelopathies: pathology and mechanisms. Acta Neuropathol. 2011;122:381–400. - PubMed
-
- Vincent A, Bien CG, Irani SR, Waters P. Autoantibodies associated with diseases of the CNS: new developments and future challenges. Lancet Neurol. 2011;10:759–772. - PubMed
-
- Tanaka M, Tanaka K, Shinozawa K, et al. Cytotoxic T cells react with recombinant Yo protein from a patient with paraneoplastic cerebellar degeneration and anti-Yo antibody. J Neurol Sci. 1998;161:88–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
