

Magnetic resonance image guided brachytherapy
- PMID: 24931089
- PMCID: PMC4147854
- DOI: 10.1016/j.semradonc.2014.02.007
Magnetic resonance image guided brachytherapy
Abstract
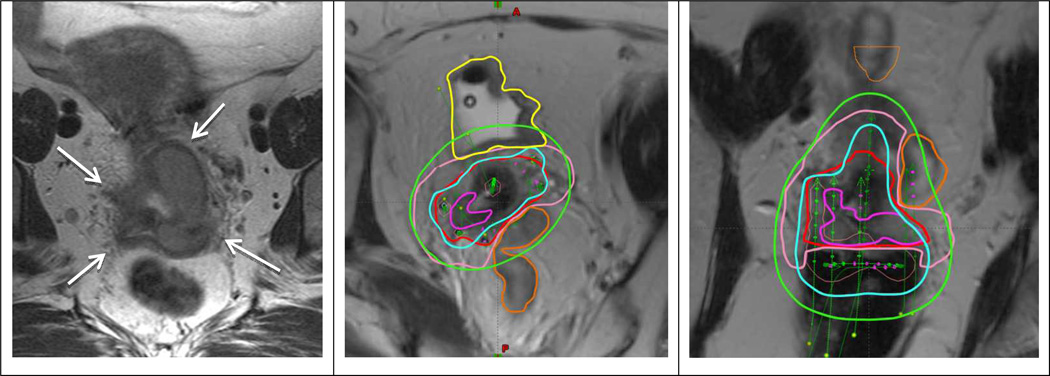
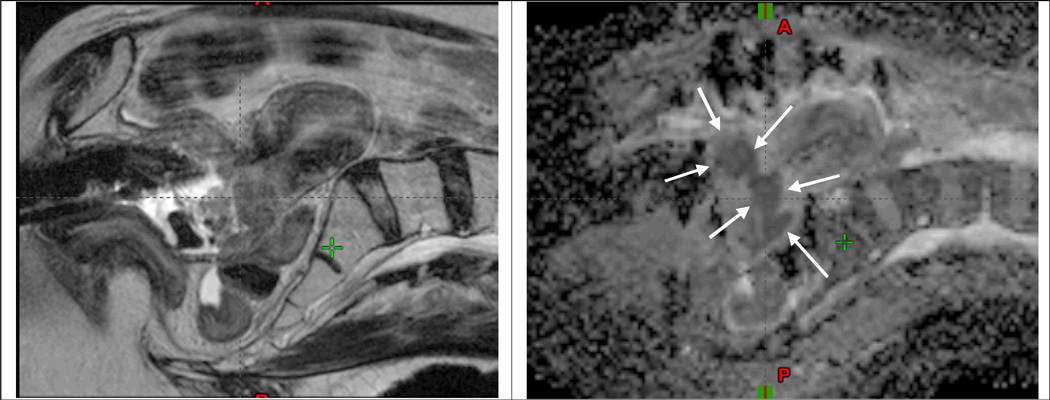
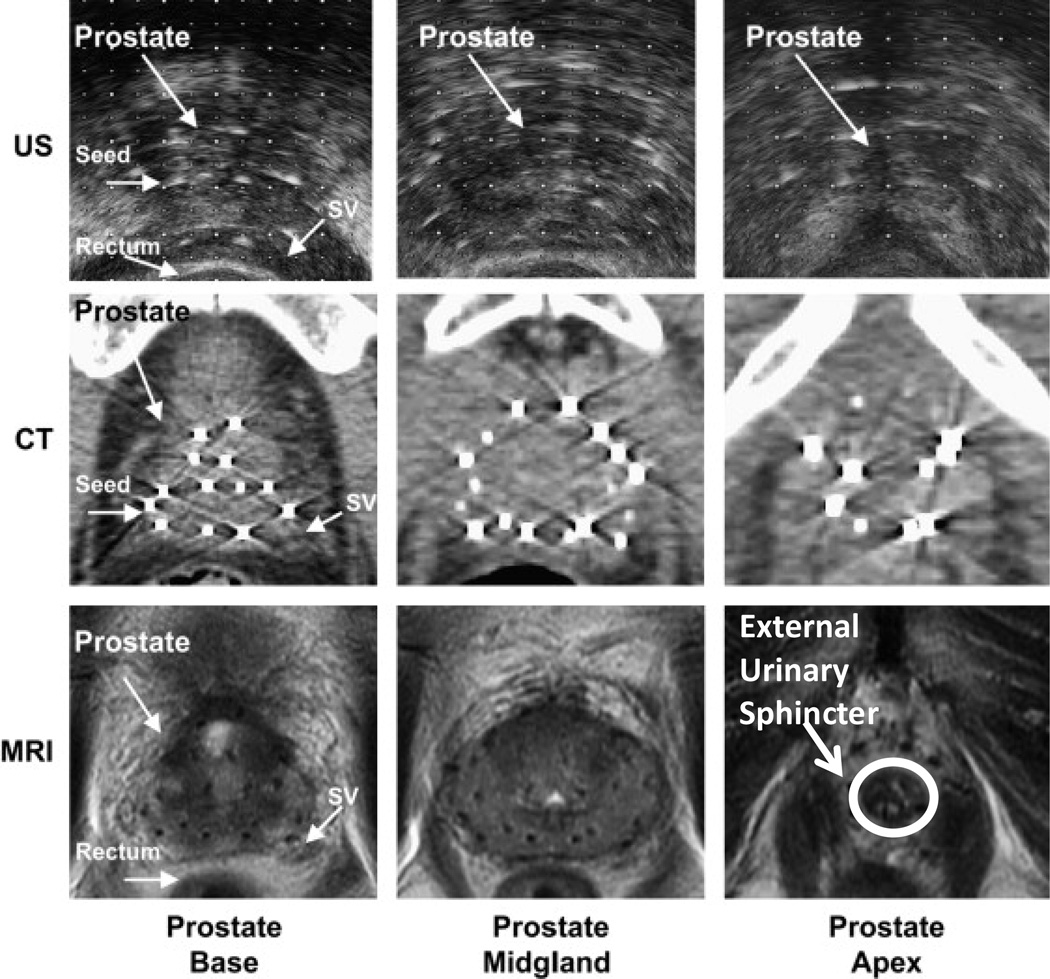
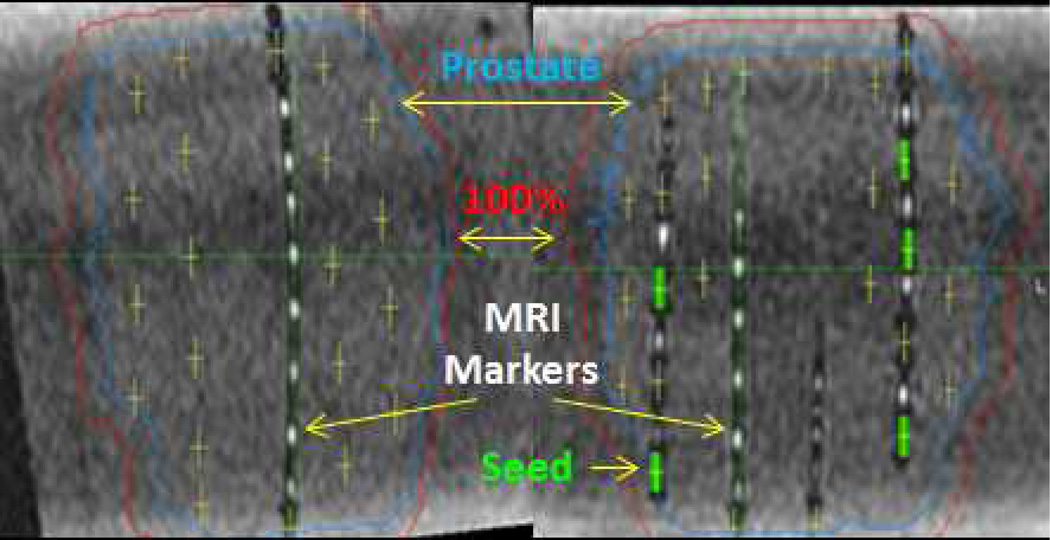
The application of magnetic resonance image (MRI)-guided brachytherapy has demonstrated significant growth during the past 2 decades. Clinical improvements in cervix cancer outcomes have been linked to the application of repeated MRI for identification of residual tumor volumes during radiotherapy. This has changed clinical practice in the direction of individualized dose administration, and resulted in mounting evidence of improved clinical outcome regarding local control, overall survival as well as morbidity. MRI-guided prostate high-dose-rate and low-dose-rate brachytherapies have improved the accuracy of target and organs-at-risk delineation, and the potential exists for improved dose prescription and reporting for the prostate gland and organs at risk. Furthermore, MRI-guided prostate brachytherapy has significant potential to identify prostate subvolumes and dominant lesions to allow for dose administration reflecting the differential risk of recurrence. MRI-guided brachytherapy involves advanced imaging, target concepts, and dose planning. The key issue for safe dissemination and implementation of high-quality MRI-guided brachytherapy is establishment of qualified multidisciplinary teams and strategies for training and education.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
References
-
- Pötter R, Dimopoulos J, Georg P, Lang S, Waldhausl C, Wachter-Gerstner N, et al. Clinical impact of MRI assisted dose volume adaptation and dose escalation in brachytherapy of locally advanced cervix cancer. Radiother Oncol. 2007 May;83(2):148–155. - PubMed
-
- Tanderup K, Nielsen SK, Nyvang GB, Pedersen EM, Rohl L, Aagaard T, et al. From point A to the sculpted pear: MR image guidance significantly improves tumour dose and sparing of organs at risk in brachytherapy of cervical cancer. Radiother Oncol. 2010 Feb;94(2):173–180. - PubMed
-
- Jürgenliemk-Schulz IM, Tersteeg RJ, Roesink JM, Bijmolt S, Nomden CN, Moerland MA, et al. MRI-guided treatment-planning optimisation in intracavitary or combined intracavitary/interstitial PDR brachytherapy using tandem ovoid applicators in locally advanced cervical cancer. Radiother Oncol. 2009 Nov;93(2):322–330. - PubMed
-
- Pötter R, Georg P, Dimopoulos JC, Grimm M, Berger D, Nesvacil N, et al. Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer. Radiother Oncol. 2011 Jul;100(1):116–123. - PMC - PubMed
-
- Lindegaard JC, Fokdal LU, Nielsen SK, Juul-Christensen J, Tanderup K. MRI-guided adaptive radiotherapy in locally advanced cervical cancer from a Nordic perspective. Acta Oncol. 2013 Oct;52(7):1510–1519. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
