

Acute and probable chronic Q fever during anti-TNFα and anti B-cell immunotherapy: a case report
- PMID: 24931640
- PMCID: PMC4065596
- DOI: 10.1186/1471-2334-14-330
Acute and probable chronic Q fever during anti-TNFα and anti B-cell immunotherapy: a case report
Abstract
Background: Q fever is caused by the intracellular bacterium Coxiella burnetii. Initial infection can present as acute Q fever, while a minority of infected individuals develops chronic Q fever endocarditis or vascular infection months to years after initial infection. Serology is an important diagnostic tool for both acute and chronic Q fever. However, since immunosuppressive drugs may hamper the humoral immune response, diagnosis of Q fever might be blurred when these drugs are used.
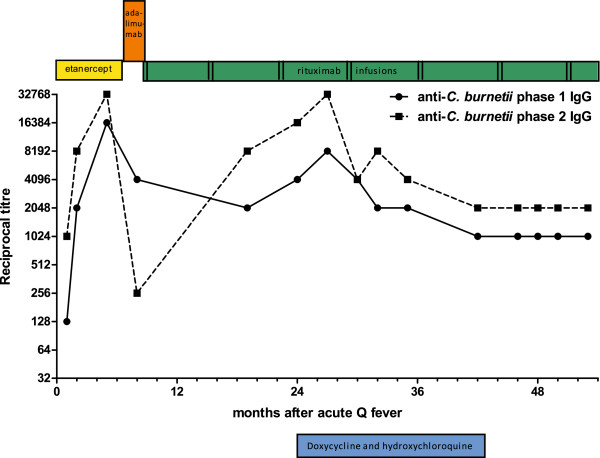
Case presentation: A 71-year-old Caucasian male was diagnosed with symptomatic acute Q fever (based on positive C. burnetii PCR followed by seroconversion) while using anti-tumor necrosis factor-α (anti-TNFα) drugs for rheumatoid arthritis (RA). He was treated for two weeks with moxifloxacin. After 24 months of follow-up, the diagnosis of probable chronic Q fever was established based on increasing anti-C. burnetii phase I IgG antibody titres in a immunocompromised patient combined with clinical suspicion of endocarditis. At the time of chronic Q fever diagnosis, he had been treated with anti B-cell therapy for 16 months. Antibiotic therapy consisting of 1.5 years doxycycline and hydroxychloroquine was started and successfully completed and no signs of relapse were seen after more than one year of follow-up.
Conclusion: The use of anti-TNFα agents for RA in the acute phase of Q fever did not hamper the C. burnetii-specific serological response as measured by immunofluorescence assay. However, in the presented case, an intact humoral response did not prevent progression to probable chronic C. burnetii infection, most likely because essential cellular immune responses were suppressed during the acute phase of the infection. Despite the start of anti-B-cell therapy with rituximab after the acute Q fever episode, an increase in anti-C. burnetii phase I IgG antibodies was observed, supporting the notion that C. burnetii specific CD20-negative memory B-cells are responsible for this rise in antibody titres.
Figures
Similar articles
-
Low antibodies titer and serological cross-reaction between Coxiella burnetii and Legionella pneumophila challenge the diagnosis of mediastinitis, an emerging Q fever clinical entity.Infection. 2017 Dec;45(6):911-915. doi: 10.1007/s15010-017-1048-6. Epub 2017 Aug 4. Infection. 2017. PMID: 28779434
-
Persistent high antibody titres against Coxiella burnetii after acute Q fever not explained by continued exposure to the source of infection: a case-control study.BMC Infect Dis. 2014 Nov 25;14:629. doi: 10.1186/s12879-014-0629-6. BMC Infect Dis. 2014. PMID: 25421141 Free PMC article.
-
Q fever in pregnant goats: humoral and cellular immune responses.Vet Res. 2013 Aug 1;44(1):67. doi: 10.1186/1297-9716-44-67. Vet Res. 2013. PMID: 23915213 Free PMC article.
-
[Acute and chronic Q fever; epidemiology, symptoms, diagnosis and therapy of infection caused by Coxiella burnetii].Ned Tijdschr Geneeskd. 2000 Jul 1;144(27):1303-6. Ned Tijdschr Geneeskd. 2000. PMID: 10918908 Review. Dutch.
-
Chronic Q fever in the United States.J Clin Microbiol. 2006 Jun;44(6):2283-7. doi: 10.1128/JCM.02365-05. J Clin Microbiol. 2006. PMID: 16757641 Free PMC article. Review.
Cited by
-
Neurotransmitter System-Targeting Drugs Antagonize Growth of the Q Fever Agent, Coxiella burnetii, in Human Cells.mSphere. 2021 Aug 25;6(4):e0044221. doi: 10.1128/mSphere.00442-21. Epub 2021 Jul 7. mSphere. 2021. PMID: 34232075 Free PMC article.
-
Q Fever Risk in Patients Treated with Chronic Antitumor Necrosis Factor-Alpha Therapy.Case Rep Infect Dis. 2016;2016:4586150. doi: 10.1155/2016/4586150. Epub 2016 Aug 30. Case Rep Infect Dis. 2016. PMID: 27656302 Free PMC article.
-
Coxiella burnetti prosthetic joint infection in an immunocompromised woman: iterative surgeries, prolonged ofloxacin-rifampin treatment and complex reconstruction were needed for the cure.Arthroplasty. 2021 Dec 2;3(1):43. doi: 10.1186/s42836-021-00097-1. Arthroplasty. 2021. PMID: 35610714 Free PMC article.
-
Homemade pericardial bifurcated graft for Q fever-infected abdominal aortic aneurysm open repair: a case report.Front Cardiovasc Med. 2024 May 28;11:1418949. doi: 10.3389/fcvm.2024.1418949. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38863900 Free PMC article.
-
Delayed diagnosis of Q fever endocarditis in a rheumatoid arthritis patient.IDCases. 2015 Sep 26;2(4):94-6. doi: 10.1016/j.idcr.2015.09.002. eCollection 2015. IDCases. 2015. PMID: 26793469 Free PMC article.
References
-
- Botelho-Nevers E, Fournier PE, Richet H, Fenollar F, Lepidi H, Foucault C, Branchereau A, Piquet P, Maurin M, Raoult D. Coxiella burnetii infection of aortic aneurysms or vascular grafts: report of 30 new cases and evaluation of outcome. Eur J Clin Microbiol Infect Dis. 2007;14(9):635–640. doi: 10.1007/s10096-007-0357-6. - DOI - PubMed
-
- Schoffelen T, Kampschreur LM, van Roeden SE, Wever PC, den Broeder AA, Nabuurs-Franssen MH, Sprong T, Joosten LA, van Riel PL, Oosterheert JJ, van Deuren M, Creemers MC. Coxiella burnetii infection (Q fever) in rheumatoid arthritis patients with and without anti-TNFα therapy. Ann Rheum Dis. 2014;14(7):1436–1438. doi: 10.1136/annrheumdis-2014-205455. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
