

Overview of surgical scar prevention and management
- PMID: 24932073
- PMCID: PMC4055805
- DOI: 10.3346/jkms.2014.29.6.751
Overview of surgical scar prevention and management
Abstract
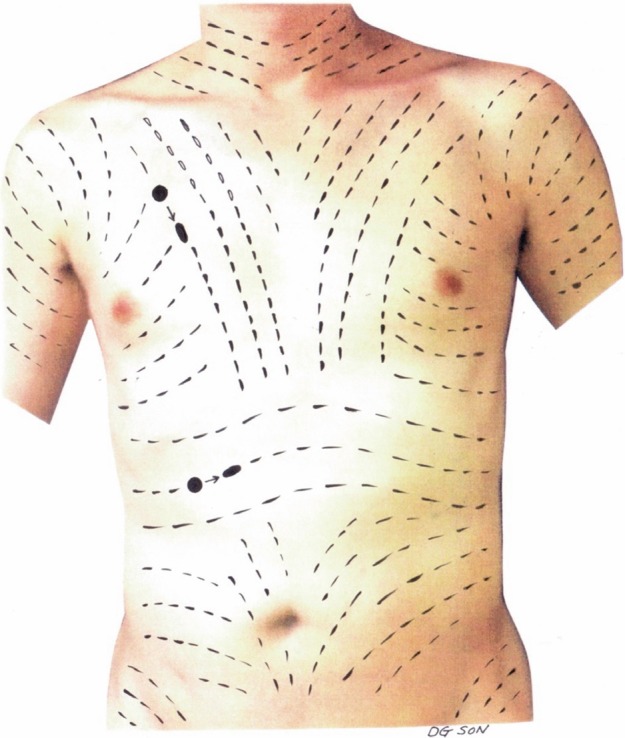
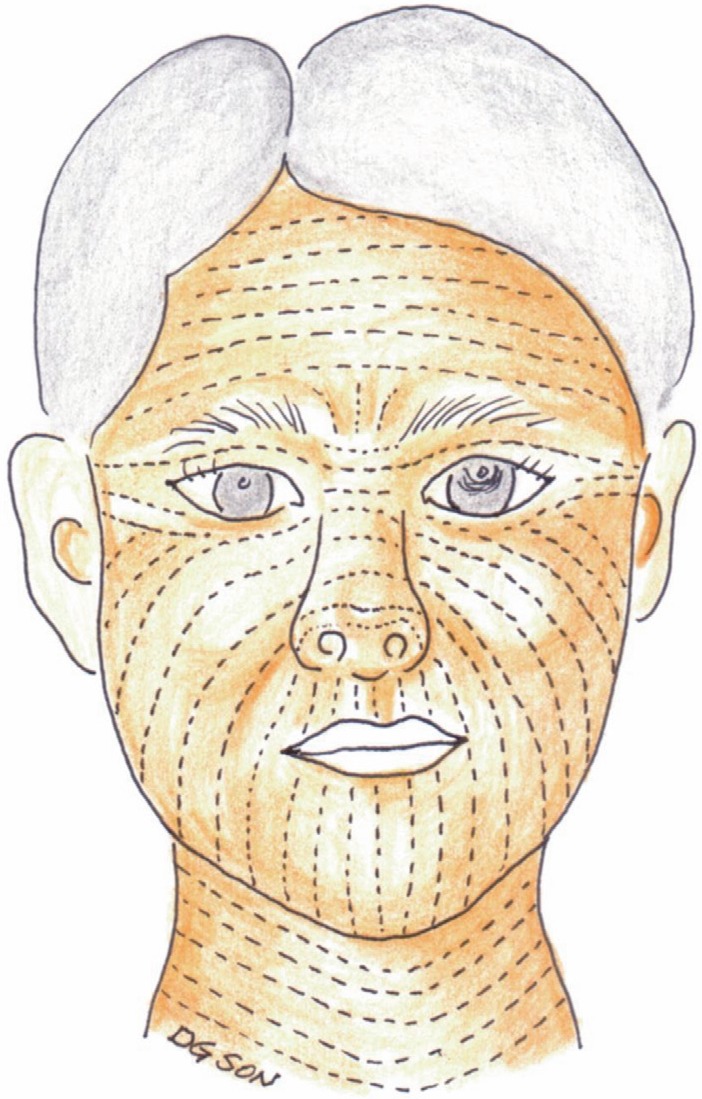
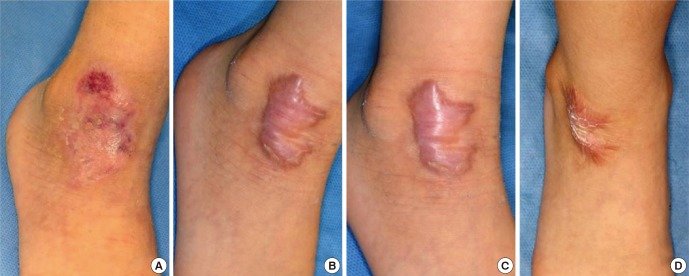
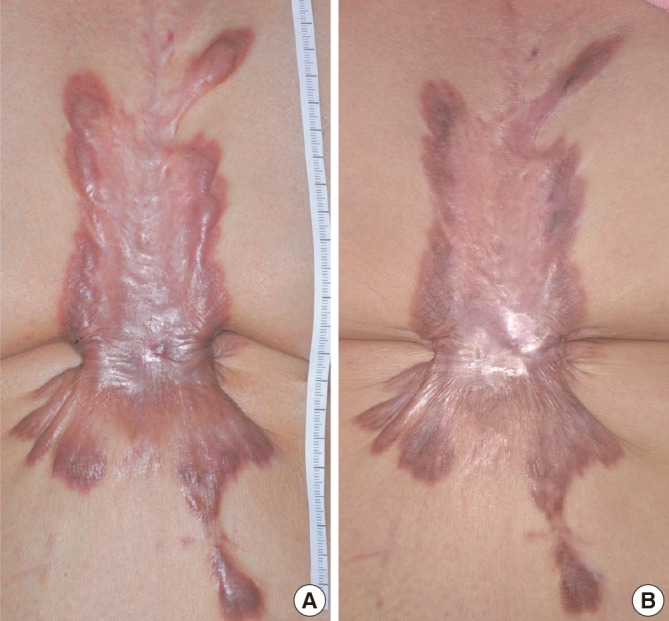
Management of incisional scar is intimately connected to stages of wound healing. The management of an elective surgery patient begins with a thorough informed consent process in which the patient is made aware of personal and clinical circumstances that cannot be modified, such as age, ethnicity, and previous history of hypertrophic scars. In scar prevention, the single most important modifiable factor is wound tension during the proliferative and remodeling phases, and this is determined by the choice of incision design. Traditional incisions most often follow relaxed skin tension lines, but no such lines exist in high surface tension areas. If such incisions are unavoidable, the patient must be informed of this ahead of time. The management of a surgical incision does not end when the sutures are removed. Surgical scar care should be continued for one year. Patient participation is paramount in obtaining the optimal outcome. Postoperative visits should screen for signs of scar hypertrophy and has a dual purpose of continued patient education and reinforcement of proper care. Early intervention is a key to control hyperplastic response. Hypertrophic scars that do not improve by 6 months are keloids and should be managed aggressively with intralesional steroid injections and alternate modalities.
Keywords: Cicatrix, Hypertrophic; Keloid; Skin Tension Line; Skin Wound Healing; Surgical Wound.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Almine JF, Wise SG, Weiss AS. Elastin signaling in wound repair. Birth Defects Res C Embryo Today. 2012;96:248–257. - PubMed
-
- Toll EC, Loizou P, Davis CR, Porter GC, Pothier DD. Scars and satisfaction: do smaller scars improve patient-reported outcome? Eur Arch Otorhinolaryngol. 2012;269:309–313. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
