

Steroid-Responsive Epilepsia Partialis Continua with Anti-Thyroid Antibodies: A Spectrum of Hashimoto's Encephalopathy?
- PMID: 24932178
- PMCID: PMC4049019
- DOI: 10.1159/000363178
Steroid-Responsive Epilepsia Partialis Continua with Anti-Thyroid Antibodies: A Spectrum of Hashimoto's Encephalopathy?
Abstract
Background: When a neuropsychiatric symptom due to encephalopathy develops in a patient with anti-thyroid antibodies, especially when the symptom is steroid-responsive, Hashimoto's encephalopathy (HE) needs to be included in the differential diagnosis of the patient. Although HE is an elusive disease, it is thought to cause various clinical presentations including seizures, myoclonus, and epilepsia partialis continua (EPC).
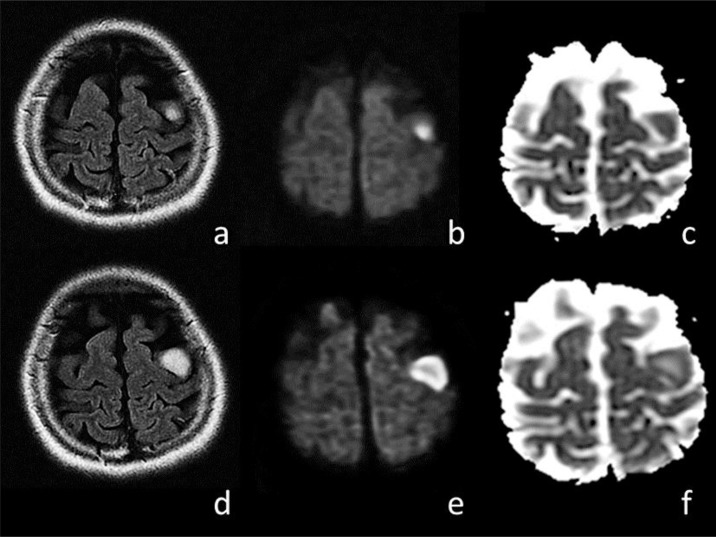
Case report: We present the case of a 33-year-old Japanese woman who acutely developed EPC in the right hand as an isolated manifestation. A thyroid ultrasound showed an enlarged hypoechogenic gland, and a thyroid status assessment showed euthyroid with high titers of thyroid antibodies. A brain MRI revealed a nodular lesion in the left precentral gyrus. Corticosteroid treatment resulted in a cessation of the symptom.
Conclusions: A precentral nodular lesion can be responsible for steroid-responsive EPC in a patient with anti-thyroid antibodies and may be caused by HE. The serial MRI findings of our case suggest the presence of primary demyelination, with ischemia possibly due to vasculitis around the demyelinating lesion.
Keywords: Demyelination; Epilepsia partialis continua; Hashimoto's disease; Hashimoto's encephalopathy; MRI; Vasculitis.
Figures
References
-
- Biraben A, Chauvel P. Epilepsia partialis continua. In: Engel J Jr, Pedley TA, editors. Epilepsy: A Comprehensive Textbook. Philadelphia: Lippincott-Raven; 1998. pp. 2447–2453.
-
- Mahad DJ, Staugaitis S, Ruggieri P, Parisi J, Kleinschmidt-Demasters BK, Lassmann H, Ransohoff RM. Steroid-responsive encephalopathy associated with autoimmune thyroiditis and primary CNS demyelination. J Neurol Sci. 2005;228:3–5. - PubMed
-
- Castillo P, Woodruff B, Caselli R, Vernino S, Lucchinetti C, Swanson J, Noseworthy J, Aksamit A, Carter J, Sirven J, Hunder G, Fatourechi V, Mokri B, Drubach D, Pittock S, Lennon V, Boeve B. Steroid-responsive encephalopathy associated with autoimmune thyroiditis. Arch Neurol. 2006;63:197–202. - PubMed
-
- Chong JY, Rowland LP, Utiger RD. Hashimoto encephalopathy: syndrome or myth? Arch Neurol. 2003;60:164–171. - PubMed
-
- Mijajlovic M, Mirkovic M, Dackovic J, Zidverc-Trajkovic J, Sternic N. Clinical manifestations, diagnostic criteria and therapy of Hashimoto's encephalopathy: report of two cases. J Neurol Sci. 2010;288:194–196. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
