

Rate and predictors of mucosal healing in patients with inflammatory bowel disease treated with anti-TNF-alpha antibodies
- PMID: 24932476
- PMCID: PMC4059645
- DOI: 10.1371/journal.pone.0099293
Rate and predictors of mucosal healing in patients with inflammatory bowel disease treated with anti-TNF-alpha antibodies
Abstract
Objective: Mucosal healing (MH) is an important treatment goal in patients with inflammatory bowel disease (IBD), but factors predicting MH under medical therapy are largely unknown. In this study, we aimed to characterize predictive factors for MH in anti-TNF-alpha antibody-treated IBD patients.
Methods: We retrospectively analyzed 248 IBD patients (61.3% CD, 38.7% UC) treated with anti-TNF-alpha antibodies (infliximab and/or adalimumab) for MH, defined as macroscopic absence of inflammatory lesions (Mayo endoscopy score 0 or SES-CD score 0) in colonoscopies which were analyzed before and after initiation of an anti-TNF-alpha antibody treatment.
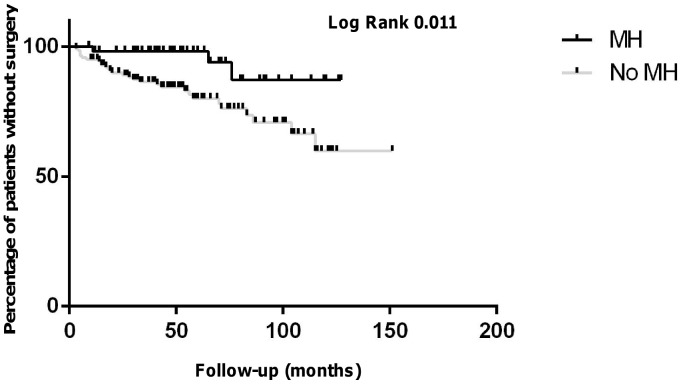
Results: In patients treated with only one anti-TNF-alpha antibody ("TNF1 group", n = 202), 56 patients (27.7%) achieved complete MH at follow-up colonoscopy (median overall follow-up time: 63 months). In a second cohort (n = 46), which comprised patients who were consecutively treated with two anti-TNF-alpha antibodies ("TNF2 group"), 13 patients (28.3%) achieved complete MH (median overall follow-up time: 64.5 months). Compared to patients without MH, CRP values at follow-up colonoscopy were significantly lower in patients with MH (TNF1 group: p = 8.35×10-5; TNF2 group: p = 0.002). Multivariate analyses confirmed CRP at follow-up colonoscopy as predictor for MH in the TNF1 group (p = 0.012). Overall need for surgery was lower in patients with MH (TNF1 group: p = 0.01; TNF2 group: p = 0.03).
Conclusions: We identified low serum CRP level at follow-up colonoscopy as predictor for MH, while MH was an excellent negative predictor for the need for surgery.
Conflict of interest statement
Figures





References
-
- Cosnes J, Gower-Rousseau C, Seksik P, Cortot A (2011) Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 140: 1785–1794. - PubMed
-
- Cosnes J, Cattan S, Blain A, Beaugerie L, Carbonnel F, et al. (2002) Long-term evolution of disease behavior of Crohn's disease. Inflamm Bowel Dis 8: 244–250. - PubMed
-
- Schroeder KW, Tremaine WJ, Ilstrup DM (1987) Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med 317: 1625–1629. - PubMed
-
- Matts SG (1961) The value of rectal biopsy in the diagnosis of ulcerative colitis. Q J Med 30: 393–407. - PubMed
-
- Lichtiger S, Present DH, Kornbluth A, Gelernt I, Bauer J, et al. (1994) Cyclosporine in severe ulcerative colitis refractory to steroid therapy. N Engl J Med 330: 1841–1845. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
