

Upper girdle imaging in facioscapulohumeral muscular dystrophy
- PMID: 24932477
- PMCID: PMC4059711
- DOI: 10.1371/journal.pone.0100292
Upper girdle imaging in facioscapulohumeral muscular dystrophy
Abstract
Background: In Facioscapulohumeral muscular dystrophy (FSHD), the upper girdle is early involved and often difficult to assess only relying on physical examination. Our aim was to evaluate the pattern and degree of involvement of upper girdle muscles in FSHD compared with other muscle diseases with scapular girdle impairment.
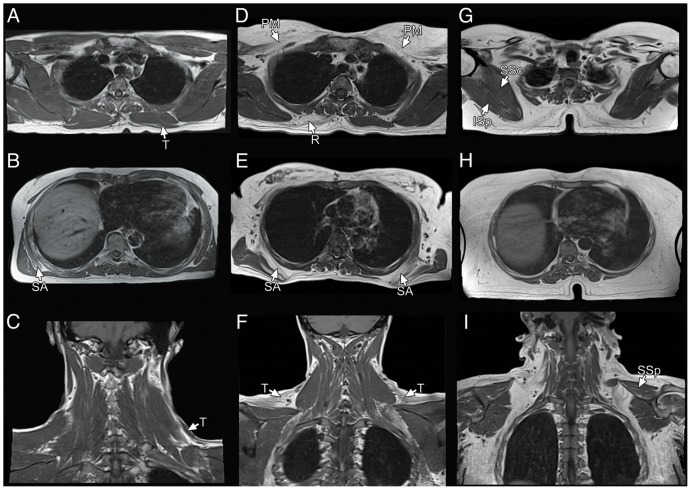
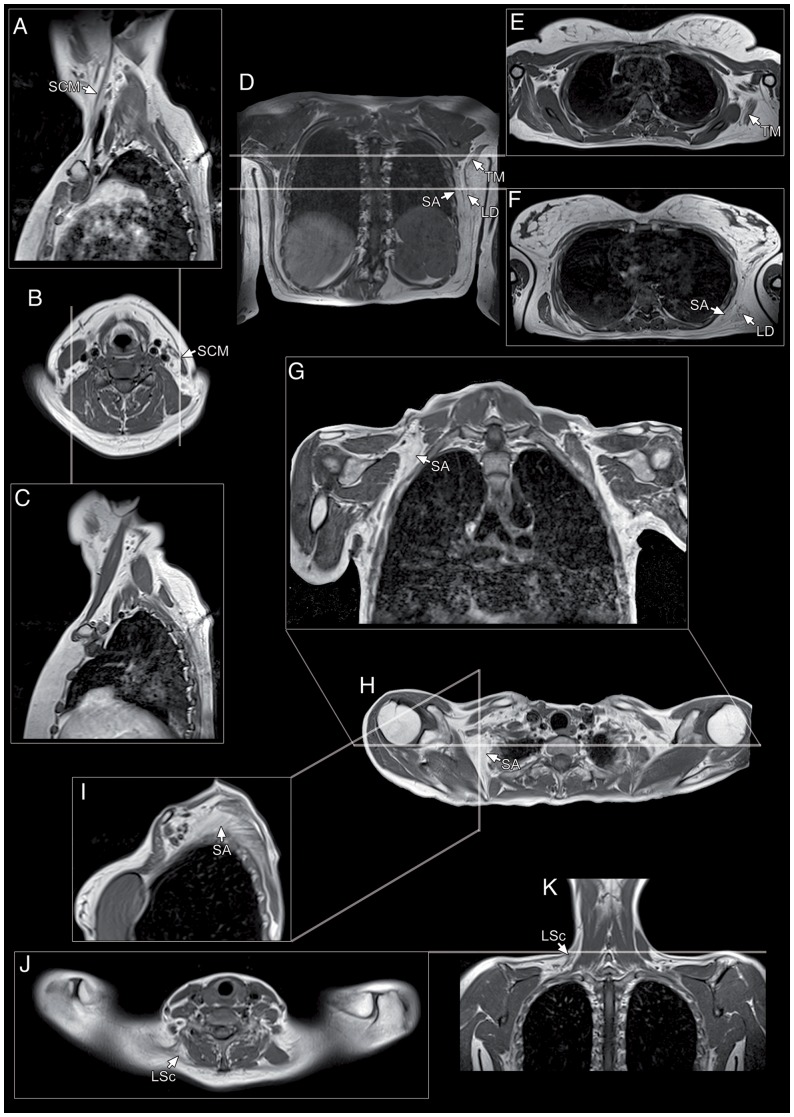
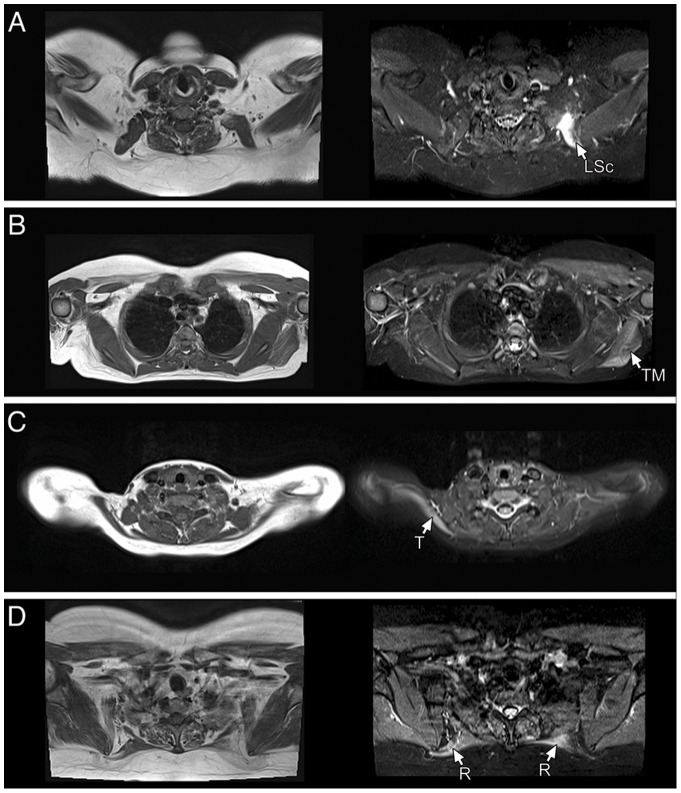
Methods: We propose an MRI protocol evaluating neck and upper girdle muscles. One hundred-eight consecutive symptomatic FSHD patients and 45 patients affected by muscular dystrophies and myopathies with prominent upper girdle involvement underwent this protocol. Acquired scans were retrospectively analyzed.
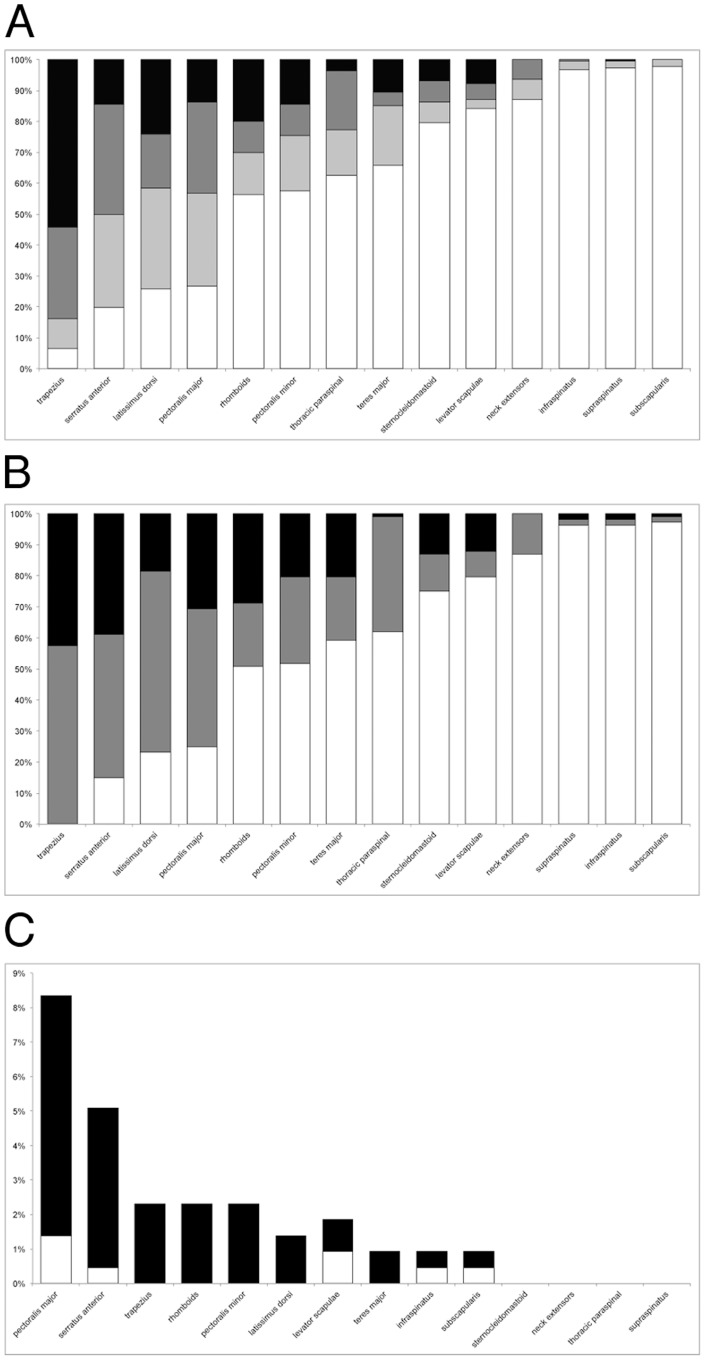
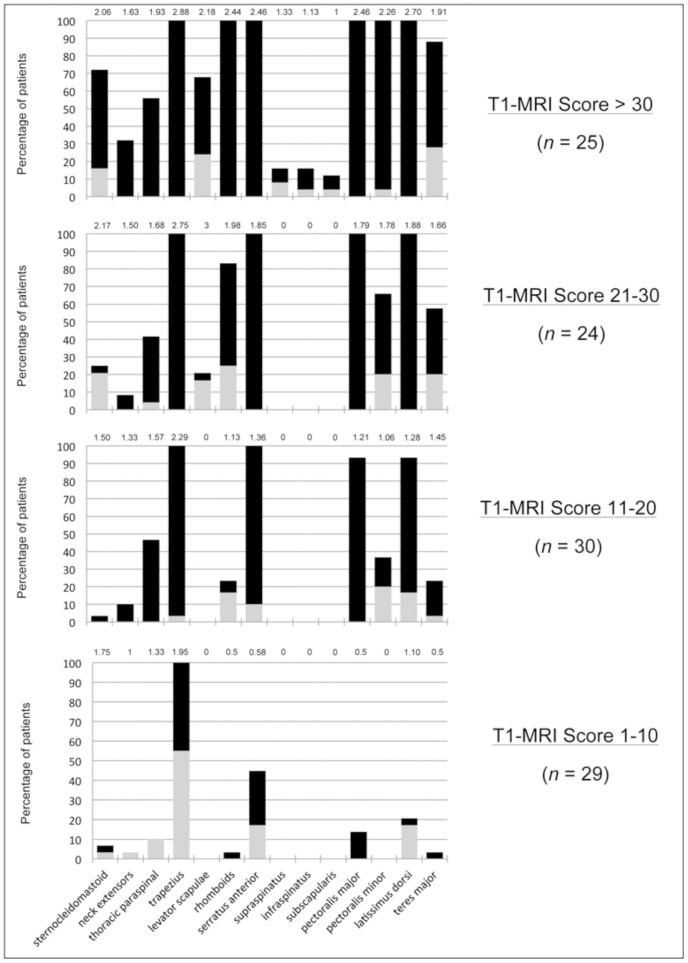
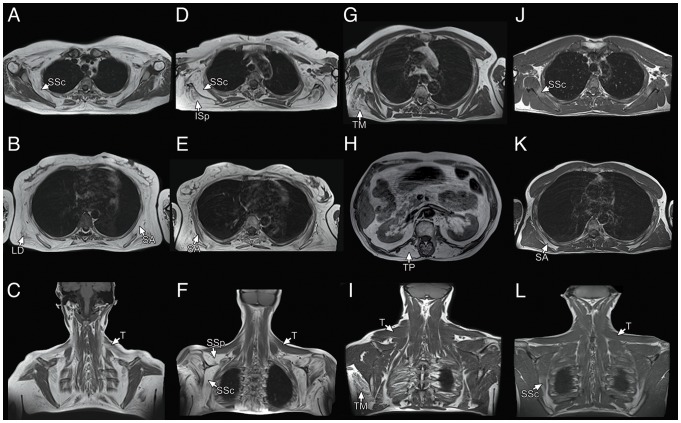
Results: The trapezius (100% of the patients) and serratus anterior (85% of the patients) were the most and earliest affected muscles in FSHD, followed by the latissimus dorsi and pectoralis major, whilst spinati and subscapularis (involved in less than 4% of the patients) were consistently spared even in late disease stages. Asymmetry and hyperintensities on short-tau inversion recovery (STIR) sequences were common features, and STIR hyperintensities could also be found in muscles not showing signs of fatty replacement. The overall involvement appears to be disease-specific in FSHD as it significantly differed from that encountered in the other myopathies.
Conclusions: The detailed knowledge of single muscle involvement provides useful information for correctly evaluating patients' motor function and to set a baseline for natural history studies. Upper girdle imaging can also be used as an additional tool helpful in supporting the diagnosis of FSHD in unclear situations, and may contribute with hints on the currently largely unknown molecular pathogenesis of this disease.
Conflict of interest statement
Figures
References
-
- Tasca G, Monforte M, Iannaccone E, Laschena F, Ottaviani P, et al. (2012) Muscle MRI in female carriers of dystrophinopathy. Eur J Neurol 19: 1256–1260. - PubMed
-
- Mercuri E, Pichiecchio A, Allsop J, Messina S, Pane M, et al. (2007) Muscle MRI in inherited neuromuscular disorders: past, present, and future. J Magn Reson Imaging 25: 433–440. - PubMed
-
- Padberg GW, van Engelen BG (2009) Facioscapulohumeral muscular dystrophy. Curr Opin Neurol 22: 539–542. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
