

Reducing unnecessary preoperative blood orders and costs by implementing an updated institution-specific maximum surgical blood order schedule and a remote electronic blood release system
- PMID: 24932853
- PMCID: PMC4165815
- DOI: 10.1097/ALN.0000000000000338
Reducing unnecessary preoperative blood orders and costs by implementing an updated institution-specific maximum surgical blood order schedule and a remote electronic blood release system
Abstract
Background: Using blood utilization data acquired from the anesthesia information management system, an updated institution-specific maximum surgical blood order schedule was introduced. The authors evaluated whether the maximum surgical blood order schedule, along with a remote electronic blood release system, reduced unnecessary preoperative blood orders and costs.
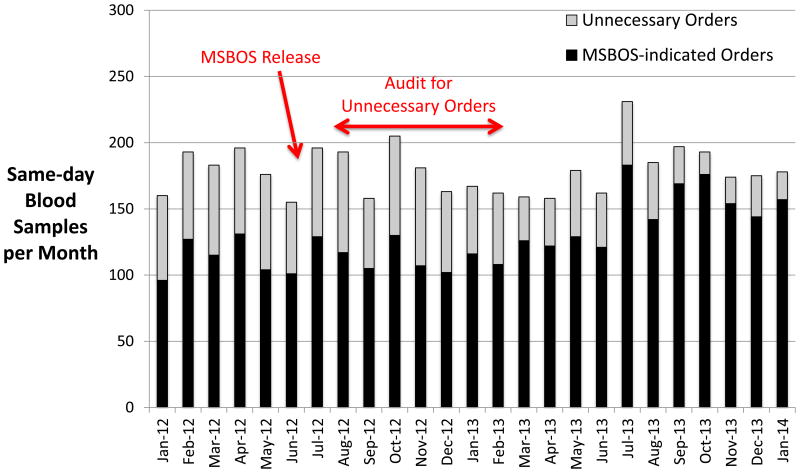
Methods: At a large academic medical center, data for preoperative blood orders were analyzed for 63,916 surgical patients over a 34-month period. The new maximum surgical blood order schedule and the electronic blood release system (Hemosafe; Haemonetics Corp., Braintree, MA) were introduced mid-way through this time period. The authors assessed whether these interventions led to reductions in unnecessary preoperative orders and associated costs.
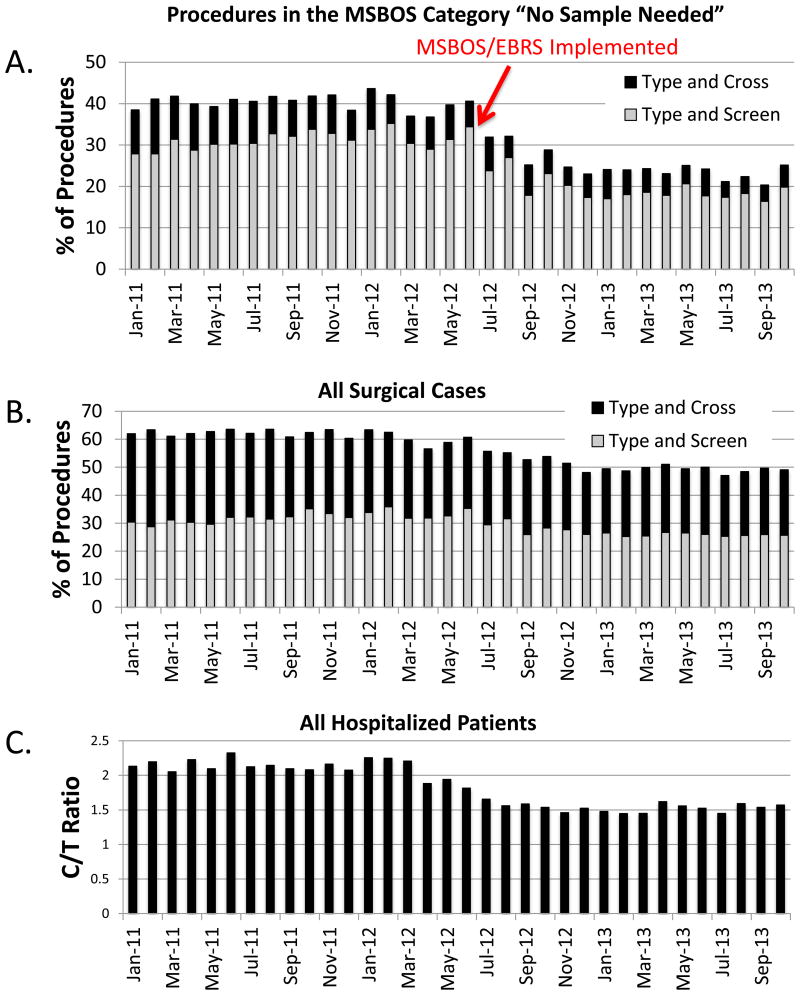
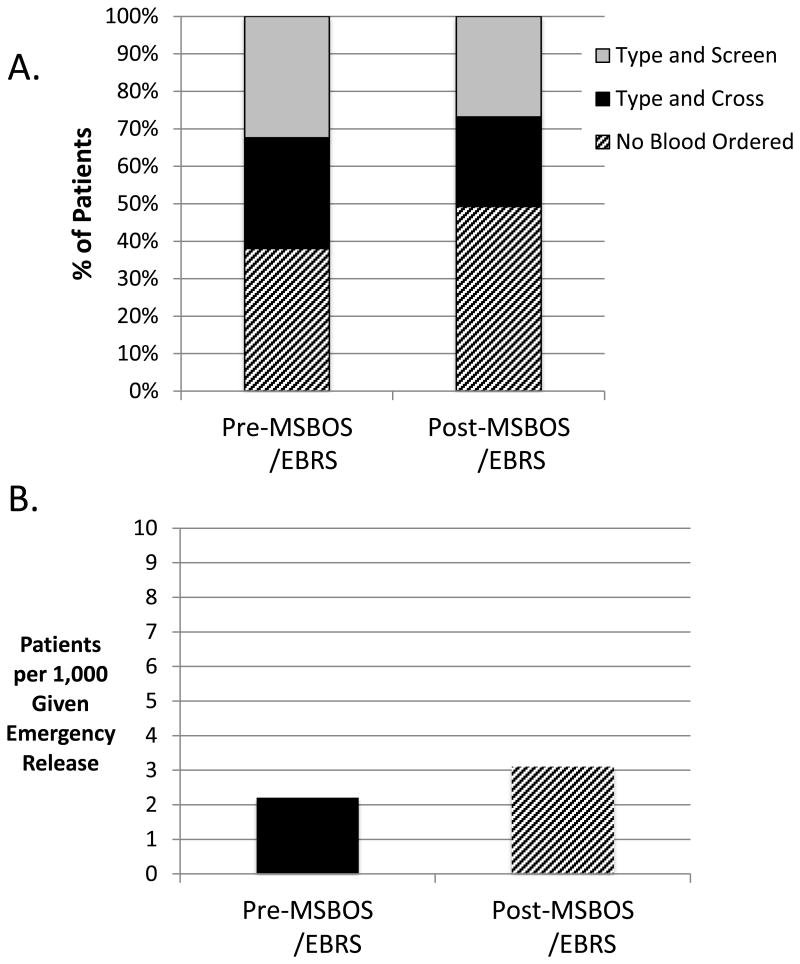
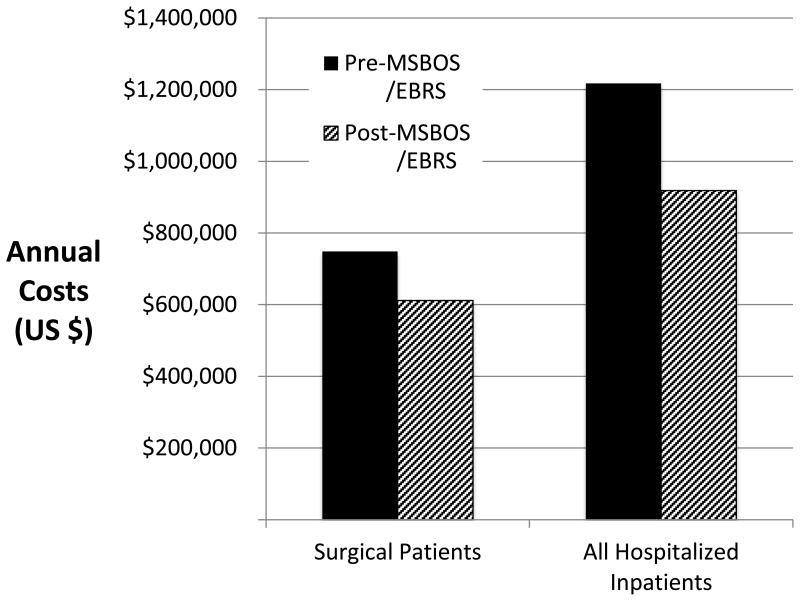
Results: Among patients having surgical procedures deemed not to require a type and screen or crossmatch (n = 33,216), the percent of procedures with preoperative blood orders decreased by 38% (from 40.4% [7,167 of 17,740 patients] to 25.0% [3,869 of 15,476 patients], P < 0.001). Among all hospitalized inpatients, the crossmatch-to-transfusion ratio decreased by 27% (from 2.11 to 1.54; P < 0.001) over the same time period. The proportion of patients who required emergency release uncrossmatched blood increased from 2.2 to 3.1 per 1,000 patients (P = 0.03); however, most of these patients were having emergency surgery. Based on the realized reductions in blood orders, annual costs were reduced by $137,223 ($6.08 per patient) for surgical patients, and by $298,966 ($6.20/patient) for all hospitalized patients.
Conclusion: Implementing institution-specific, updated maximum surgical blood order schedule-directed preoperative blood ordering guidelines along with an electronic blood release system results in a substantial reduction in unnecessary orders and costs, with a clinically insignificant increase in requirement for emergency release blood transfusions.
Figures
References
-
- American Society of Anesthesiologists Task Force on Perioperative Blood T, Adjuvant T. Practice guidelines for perioperative blood transfusion and adjuvant therapies: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiology. 2006;105:198–208. - PubMed
-
- Napolitano LM, Kurek S, Luchette FA, Anderson GL, Bard MR, Bromberg W, Chiu WC, Cipolle MD, Clancy KD, Diebel L, Hoff WS, Hughes KM, Munshi I, Nayduch D, Sandhu R, Yelon JA, Corwin HL, Barie PS, Tisherman SA, Hebert PC, Workgroup EPM. American College of Critical Care Medicine Taskforce of the Society of Critical Care Medicine: Clinical practice guideline: Red blood cell transfusion in adult trauma and critical care. J Trauma. 2009;67:1439–42. - PubMed
-
- Carson JL, Grossman BJ, Kleinman S, Tinmouth AT, Marques MB, Fung MK, Holcomb JB, Illoh O, Kaplan LJ, Katz LM, Rao SV, Roback JD, Shander A, Tobian AA, Weinstein R, Swinton McLaughlin LG, Djulbegovic B. Clinical Transfusion Medicine Committee of the AABB: Red blood cell transfusion: A clinical practice guideline from the AABB*. Ann Intern Med. 2012;157:49–58. - PubMed
-
- Society of Thoracic Surgeons Blood Conservation Guideline Task Force. Ferraris VA, Brown JR, Despotis GJ, Hammon JW, Reece TB, Saha SP, Song HK, Clough ER, Society of Cardiovascular Anesthesiologists Special Task Force on Blood Transfusion. Shore-Lesserson LJ, Goodnough LT, Mazer CD, Shander A, Stafford-Smith M, Waters J, International Consortium for Evidence Based Perfusion. Baker RA, Dickinson TA, FitzGerald DJ, Likosky DS, Shann KG. 2011 Update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists blood conservation clinical practice guidelines. Ann Thorac Surg. 2011;91:944–82. - PubMed
-
- Mintz PD, Nordine RB, Henry JB, Webb WR. Expected hemotherapy in elective surgery. N Y State J Med. 1976;76:532–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
