

On improving the use of OCT imaging for detecting glaucomatous damage
- PMID: 24934219
- PMCID: PMC4208344
- DOI: 10.1136/bjophthalmol-2014-305156
On improving the use of OCT imaging for detecting glaucomatous damage
Abstract
Aims: To describe two approaches for improving the detection of glaucomatous damage seen with optical coherence tomography (OCT).
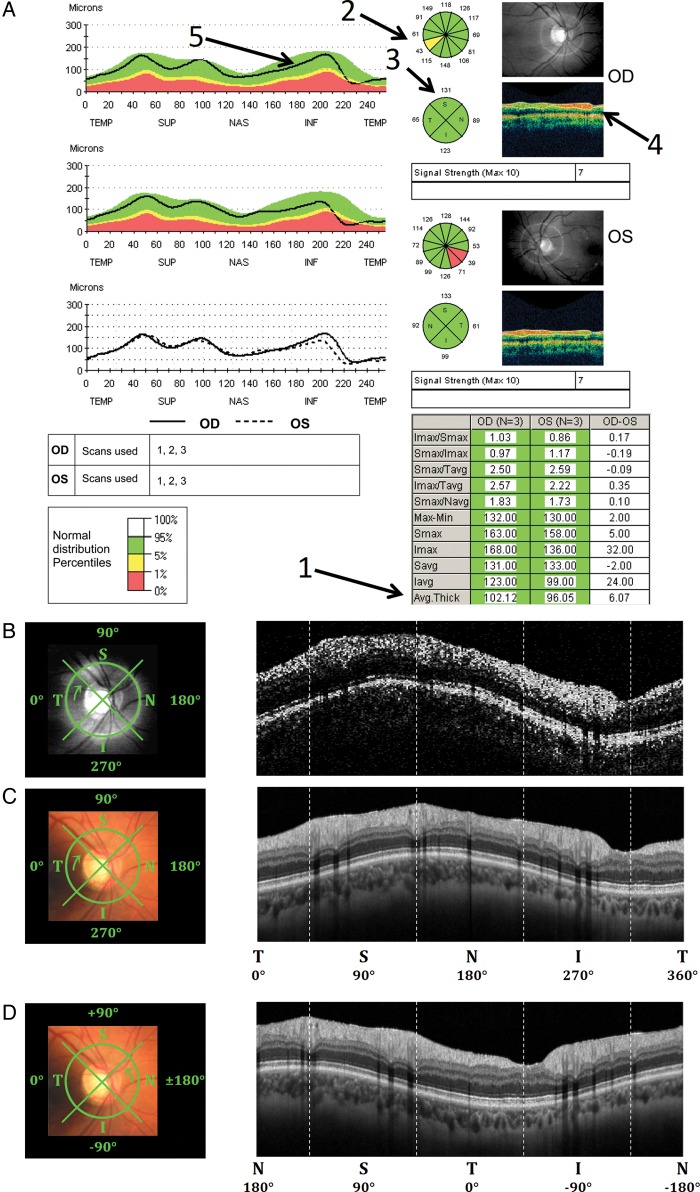
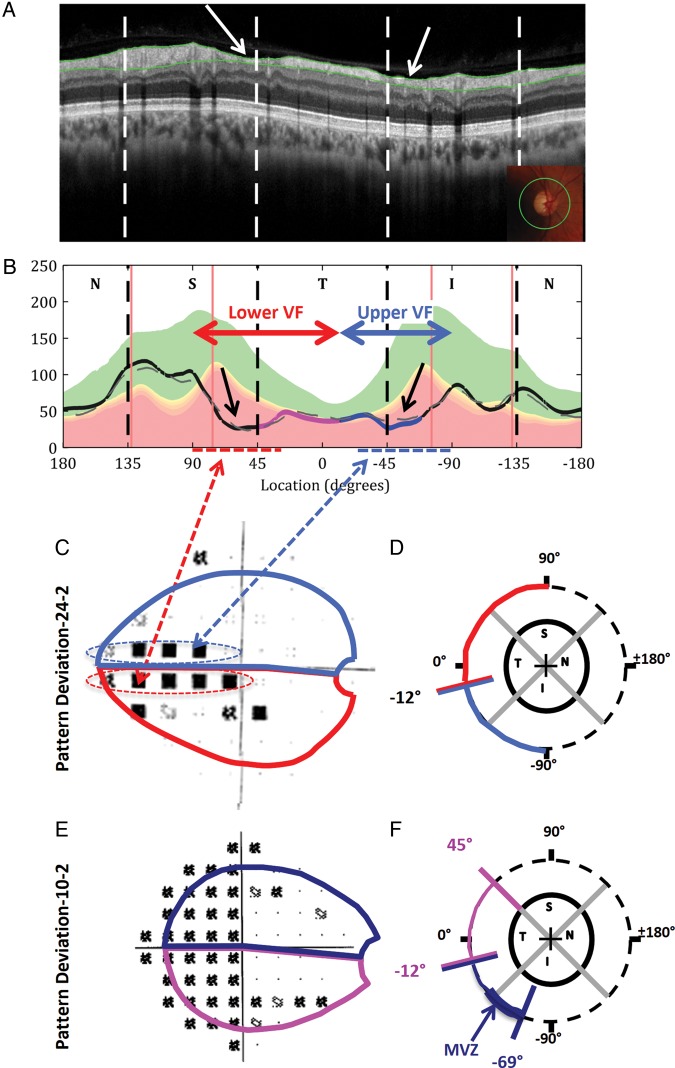
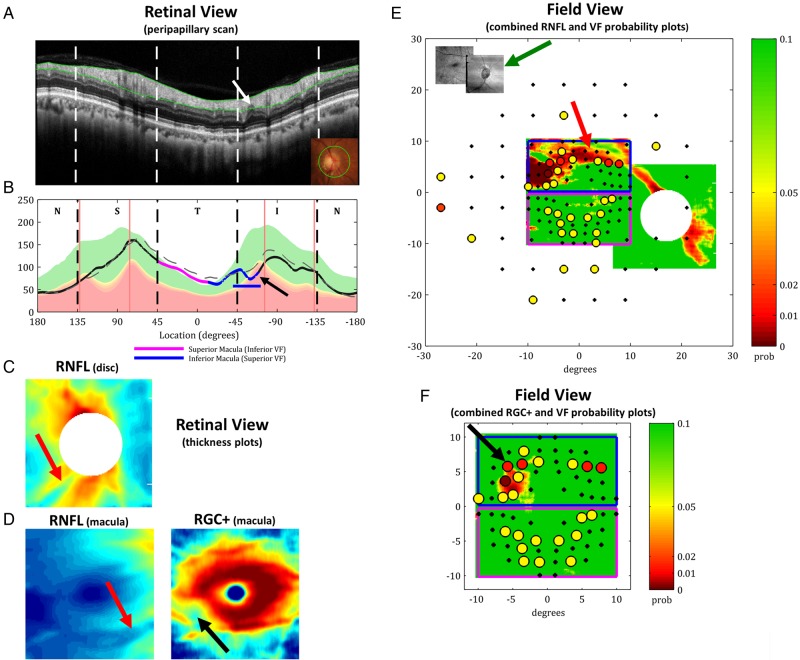
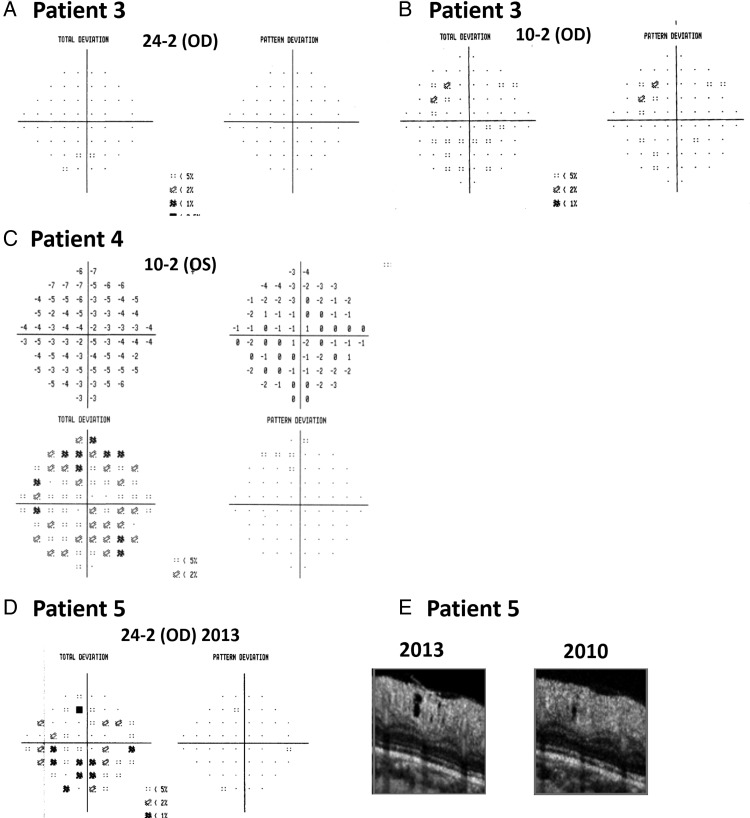
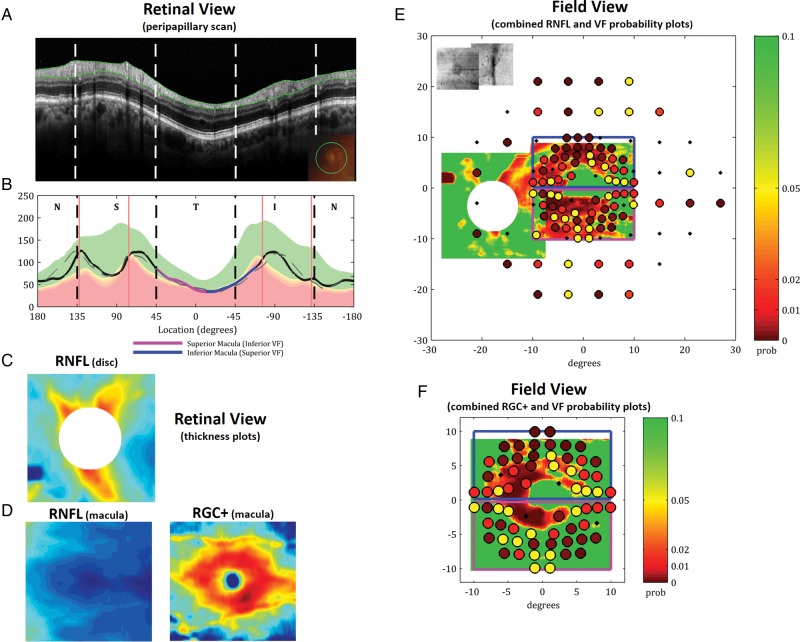
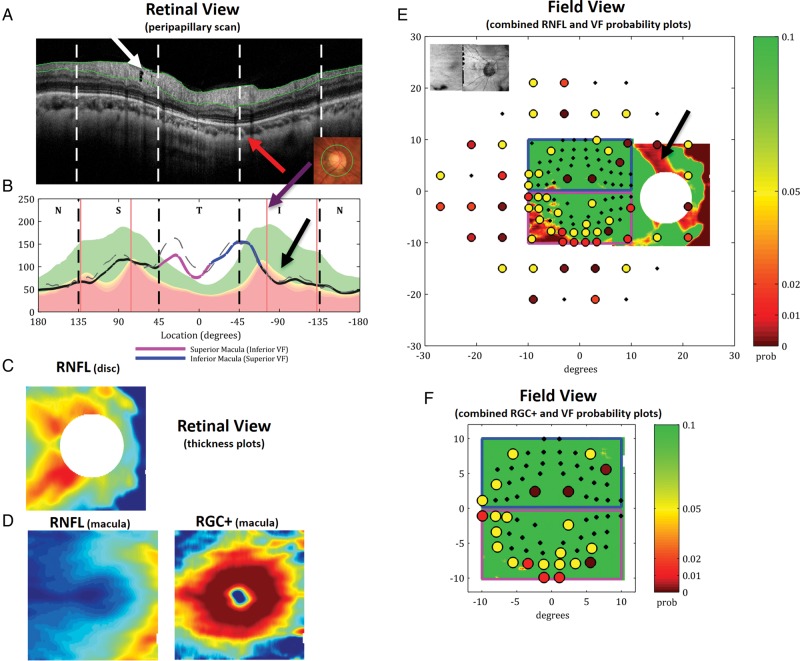
Methods: The two approaches described were: one, a visual analysis of the high-quality OCT circle scans and two, a comparison of local visual field sensitivity loss to local OCT retinal ganglion cell plus inner plexiform (RGC+) and retinal nerve fibre layer (RNFL) thinning. OCT images were obtained from glaucoma patients and suspects using a spectral domain OCT machine and commercially available scanning protocols. A high-quality peripapillary circle scan (average of 50), a three-dimensional (3D) scan of the optic disc, and a 3D scan of the macula were obtained. RGC+ and RNFL thickness and probability plots were generated from the 3D scans.
Results: A close visual analysis of a high-quality circle scan can help avoid both false positive and false negative errors. Similarly, to avoid these errors, the location of abnormal visual field points should be compared to regions of abnormal RGC+ and RNFL thickness.
Conclusions: To improve the sensitivity and specificity of OCT imaging, high-quality images should be visually scrutinised and topographical information from visual fields and OCT scans combined.
Keywords: Glaucoma; Imaging; Optic Nerve; Psychophysics.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical