

Robotic thyroidectomy for cancer in the US: patterns of use and short-term outcomes
- PMID: 24934584
- PMCID: PMC4519825
- DOI: 10.1245/s10434-014-3838-8
Robotic thyroidectomy for cancer in the US: patterns of use and short-term outcomes
Abstract
Background: We describe nationally representative patterns of utilization and short-term outcomes from robotic versus open thyroidectomy for thyroid cancer.
Methods: Descriptive statistics and multivariable analysis were used to analyze patterns of use of robotic thyroidectomy from the National Cancer Database (2010-2011). Short-term outcomes were compared between patients undergoing robotic versus open thyroidectomy, while adjusting for confounders.
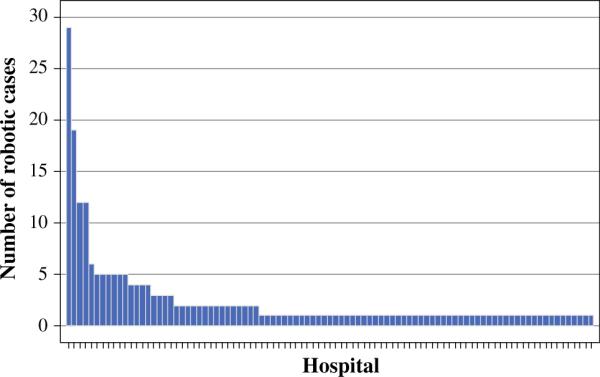
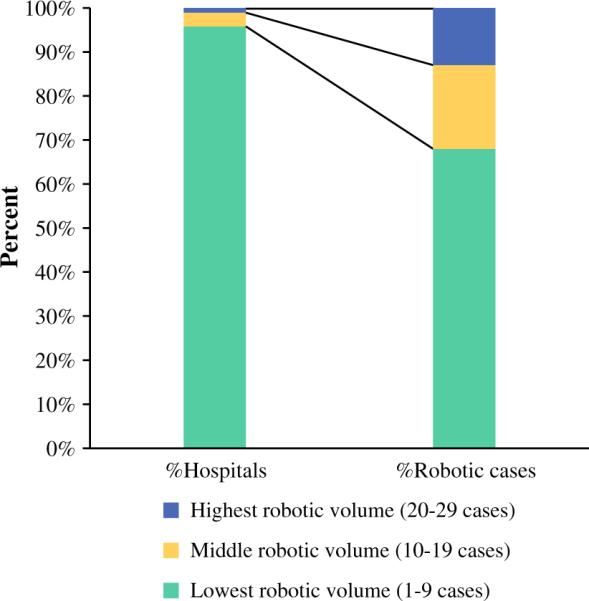
Results: A total of 68,393 patients with thyroid cancer underwent thyroidectomy; 225 had robotic surgery and 57,729 underwent open surgery. Robotic thyroid surgery use increased by 30 % from 2010 to 2011 (p = 0.08). Robotic cases were reported from 93 centers, with 89 centers performing <10 robotic cases. Compared with the open group, the robotic group was younger (51 vs. 47 years; p < 0.01) and included more Asian patients (4 vs. 8 %; p = 0.006) and privately-insured patients (68 vs. 77 %; p = 0.01). Tumor size was similar between patients undergoing robotic versus open surgery. Total thyroidectomy was performed less frequently in the robotic group (67 vs. 84 % open; p < 0.0001). Patients were relatively more likely to undergo robotic surgery if they were female (odds ratio [OR] 1.6; p = 0.04), younger (OR 0.8/10 years; p < 0.0001), or underwent lobectomy (OR 2.4; p < 0.0001). In adjusted multivariable analysis, there were no differences in the number of lymph nodes removed or length of stay between groups; however, there was a non-significant increase in the incidence of positive margins with robotic thyroidectomy.
Conclusions: Use of robotic thyroidectomy for thyroid cancer is limited to a few institutions, with short-term outcomes that are comparable to open surgery. Multi-institutional studies should be undertaken to compare thyroidectomy-specific complications and long-term outcomes.
Figures
References
-
- Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014;140(4):317–22. - PubMed
-
- American Cancer Society [1 Mar 2014];Cancer facts & figures. 2013 http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/docume....
-
- Shaha AR. Implications of prognostic factors and risk groups in the management of differentiated thyroid cancer. Laryngoscope. 2004;114(3):393–402. - PubMed
-
- Hannan SA. The magnificent seven: a history of modern thyroid surgery. Int J Surg. 2006;4(3):187–91. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
