

Candida colonization index and subsequent infection in critically ill surgical patients: 20 years later
- PMID: 24934813
- PMCID: PMC4176828
- DOI: 10.1007/s00134-014-3355-z
Candida colonization index and subsequent infection in critically ill surgical patients: 20 years later
Abstract
Introduction: For decades, clinicians dealing with immunocompromised and critically ill patients have perceived a link between Candida colonization and subsequent infection. However, the pathophysiological progression from colonization to infection was clearly established only through the formal description of the colonization index (CI) in critically ill patients. Unfortunately, the literature reflects intense confusion about the pathophysiology of invasive candidiasis and specific associated risk factors.
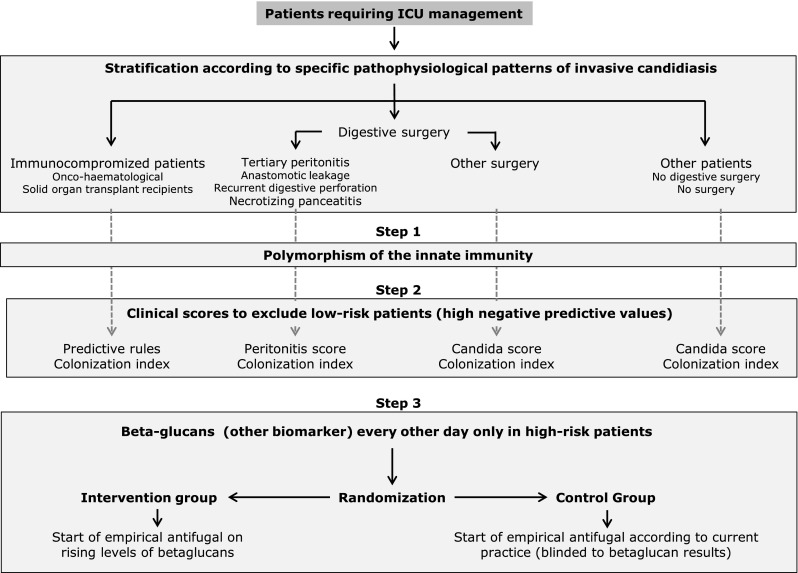
Methods: We review the contribution of the CI in the field of Candida infection and its development in the 20 years following its original description in 1994. The development of the CI enabled an improved understanding of the pathogenesis of invasive candidiasis and the use of targeted empirical antifungal therapy in subgroups of patients at increased risk for infection.
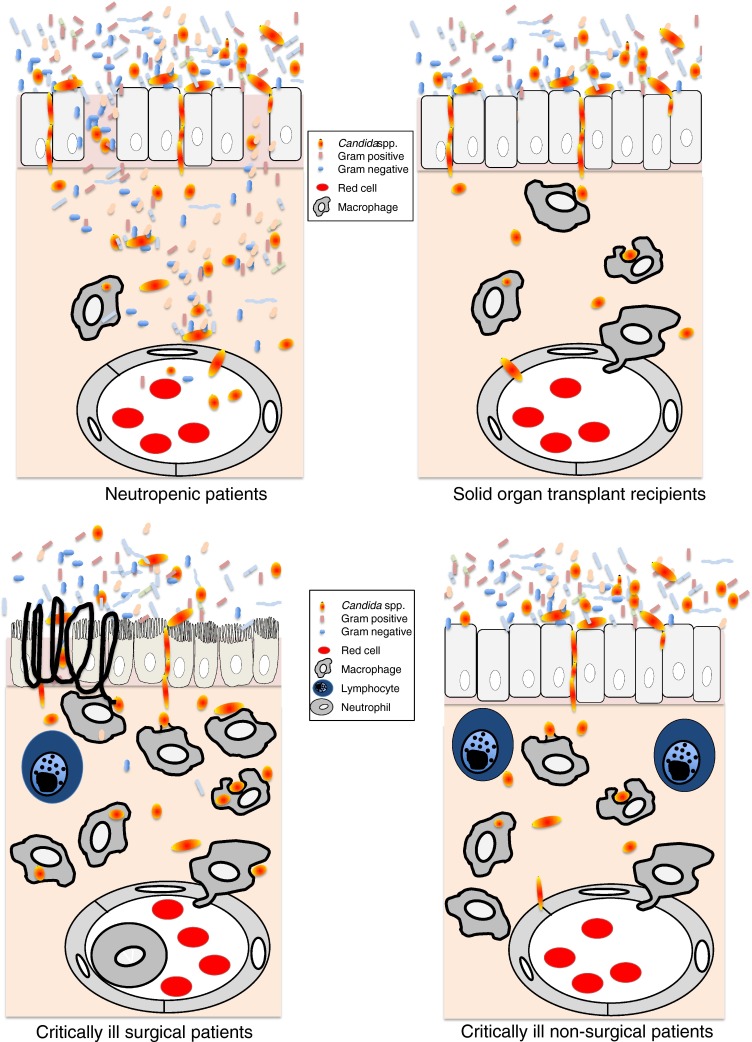
Results: The recognition of specific characteristics among underlying conditions, such as neutropenia, solid organ transplantation, and surgical and nonsurgical critical illness, has enabled the description of distinct epidemiological patterns in the development of invasive candidiasis.
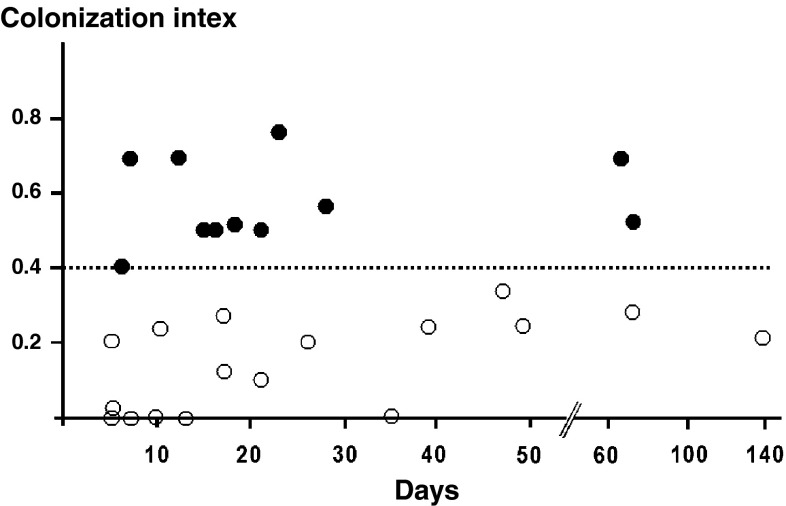
Conclusions: Despite its limited bedside practicality and before confirmation of potentially more accurate predictors, such as specific biomarkers, the CI remains an important way to characterize the dynamics of colonization, which increases early in patients who develop invasive candidiasis.
Figures
References
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K, EPIC II Group of Investigators International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323–2329. doi: 10.1001/jama.2009.1754. - DOI - PubMed
-
- Pfaller M, Neofytos D, Diekema D, Azie N, Meier-Kriesche HU, Quan SP, Horn D. Epidemiology and outcomes of candidemia in 3648 patients: data from the Prospective Antifungal Therapy (PATH Alliance®) registry, 2004-2008. Diagn Microbiol Infect Dis. 2012;74:323–331. doi: 10.1016/j.diagmicrobio.2012.10.003. - DOI - PubMed
-
- Guery BP, Arendrup MC, Auzinger G, Azoulay E, Borges Sa M, Johnson EM, Muller E, Putensen C, Rotstein C, Sganga G, Venditti M, Zaragoza Crespo R, Kullberg BJ. Management of invasive candidiasis and candidemia in adult non-neutropenic intensive care unit patients: part I. Epidemiology and diagnosis. Intensive Care Med. 2009;35:55–62. doi: 10.1007/s00134-008-1338-7. - DOI - PubMed
-
- Kett DH, Azoulay E, Echeverria PM, Vincent JL, Extended Prevalence of Infection in ICUSGoI Candida bloodstream infections in intensive care units: analysis of the extended prevalence of infection in intensive care unit study. Crit Care Med. 2011;39:665–670. doi: 10.1097/CCM.0b013e318206c1ca. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
