

Systolic blood pressure levels among adults with hypertension and incident cardiovascular events: the atherosclerosis risk in communities study
- PMID: 24935209
- PMCID: PMC4573449
- DOI: 10.1001/jamainternmed.2014.2482
Systolic blood pressure levels among adults with hypertension and incident cardiovascular events: the atherosclerosis risk in communities study
Erratum in
- JAMA Intern Med. 2014 Aug;174(8):1419
Abstract
Importance: Studies document a progressive increase in heart disease risk as systolic blood pressure (SBP) rises above 115 mm Hg, but it is unknown whether an SBP lower than 120 mm Hg among adults with hypertension (HTN) lowers heart failure, stroke, and myocardial infarction risk.
Objective: To examine the risk of incident cardiovascular (CV) events among adults with HTN according to 3 SBP levels: 140 mm Hg or higher; 120 to 139 mm Hg; and a reference level of lower than 120 mm Hg.
Design, setting, and participants: A total of 4480 participants with HTN but without prevalent CV disease at baseline (years 1987-1989) from the Atherosclerosis Risk in Communities Study were included. Measurements of SBP were taken at baseline and at 3 triennial visits; SBP was treated as a time-dependent variable and categorized as elevated (≥140 mm Hg), standard (120-139 mm Hg), and low (<120 mm Hg). Multivariable Cox regression models included baseline age, sex, diabetes status, BMI, high cholesterol level, smoking status, and alcohol intake.
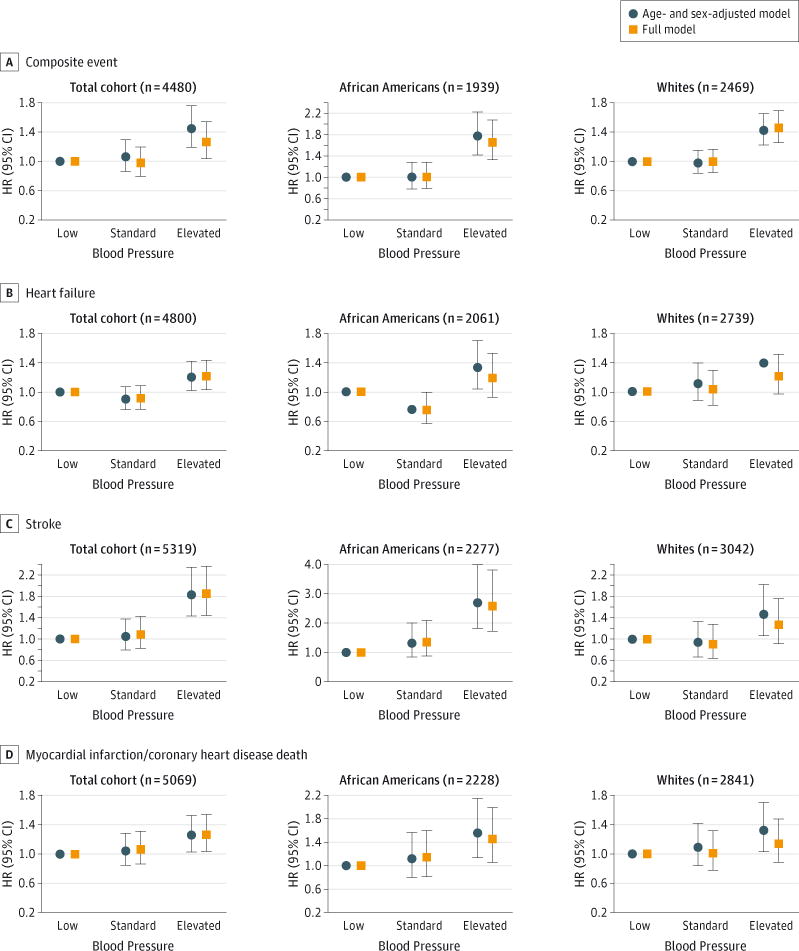
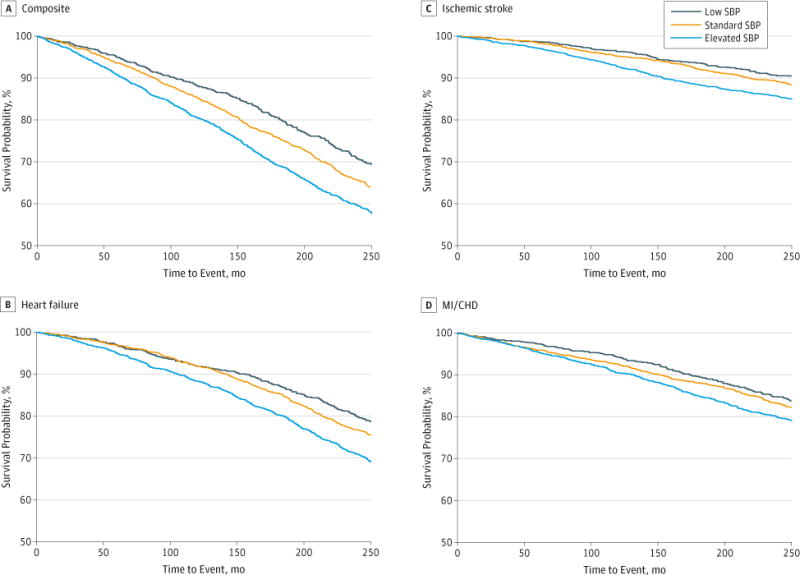
Main outcomes and measures: Incident composite CV events (heart failure, ischemic stroke, myocardial infarction, or death related to coronary heart disease).
Results: After a median follow-up of 21.8 years, a total of 1622 incident CV events had occurred. Participants with elevated SBP developed incident CV events at a significantly higher rate than those in the low BP group (adjusted hazard ratio [HR], 1.46; 95% CI, 1.26-1.69). However, there was no difference in incident CV event-free survival among those in the standard vs low SBP group (adjusted HR, 1.00; 95% CI, 0.85-1.17). Further adjustment for BP medication use or diastolic BP did not significantly affect the results.
Conclusions and relevance: Among patients with HTN, having an elevated SBP carries the highest risk for cardiovascular events, but in this categorical analysis, once SBP was below 140 mm Hg, an SBP lower than 120 mm Hg did not appear to lessen the risk of incident CV events.
Conflict of interest statement
Conflict of Interest Disclosures: None reported.
Figures
Comment in
-
Let's prioritize the right care for the right patients with hypertension.JAMA Intern Med. 2014 Aug;174(8):1261-2. doi: 10.1001/jamainternmed.2014.1000. JAMA Intern Med. 2014. PMID: 24934360 No abstract available.
-
Aiming too high or too low? Searching for the appropriate therapeutic thresholds in hypertension is not over yet.Evid Based Med. 2015 Feb;20(1):27. doi: 10.1136/ebmed-2014-110104. Epub 2014 Dec 8. Evid Based Med. 2015. PMID: 25488933 No abstract available.
References
-
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC-8) JAMA. 2014;311(5):507–520. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. - PubMed
-
- Lawes CM, Vander Hoorn S, Rodgers A, International Society of Hypertension Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371(9623):1513–1518. - PubMed
-
- The ARIC Investigators. The Atherosclerosis Risk in Communities (ARIC) Study: design and objectives. Am J Epidemiol. 1989;129(4):687–702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- R01 HL104199/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
