

Comparison of clinical and biochemical markers of dehydration with the clinical dehydration scale in children: a case comparison trial
- PMID: 24935348
- PMCID: PMC4081489
- DOI: 10.1186/1471-2431-14-149
Comparison of clinical and biochemical markers of dehydration with the clinical dehydration scale in children: a case comparison trial
Abstract
Background: The clinical dehydration scale (CDS) is a quick, easy-to-use tool with 4 clinical items and a score of 1-8 that serves to classify dehydration in children with gastroenteritis as no, some or moderate/severe dehydration. Studies validating the CDS (Friedman JN) with a comparison group remain elusive. We hypothesized that the CDS correlates with a wide spectrum of established markers of dehydration, making it an appropriate and easy-to-use clinical tool.
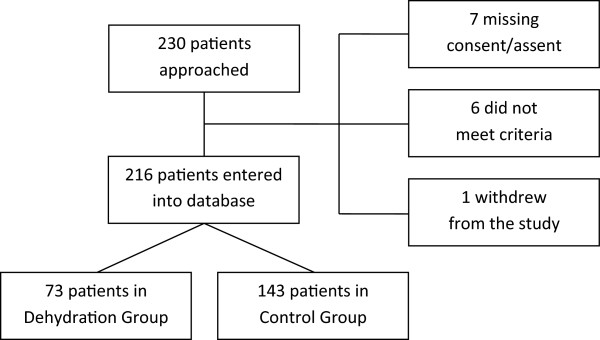
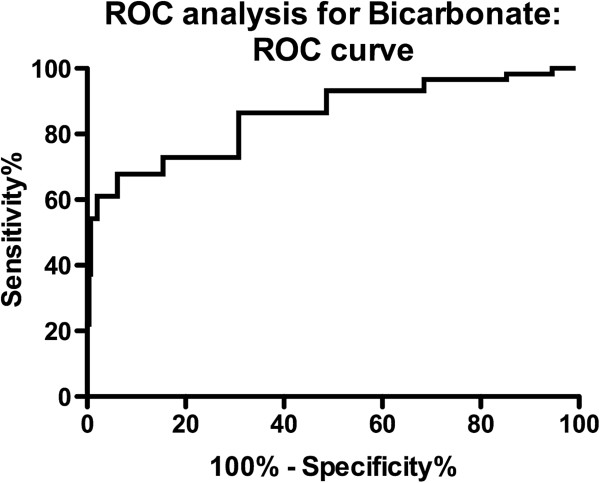
Methods: This study was designed as a prospective double-cohort trial in a single tertiary care center. Children with diarrhea and vomiting, who clinically required intravenous fluids for rehydration, were compared with minor trauma patients who required intravenous needling for conscious sedation. We compared the CDS with clinical and urinary markers (urinary electrolytes, proteins, ratios and fractional excretions) for dehydration in both groups using receiver operating characteristic (ROC) curves to determine the area under the curve (AUC).
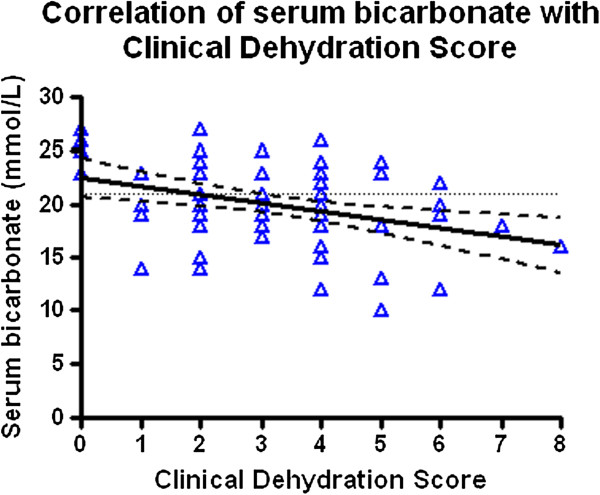
Results: We enrolled 73 children (male = 36) in the dehydration group and 143 (male = 105) in the comparison group. Median age was 32 months (range 3-214) in the dehydration and 96 months (range 2.6-214 months, p < 0.0001) in the trauma group. Median CDS was 3 (range 0-8) within the dehydration group and 0 in the comparison group (p < 0.0001). The following parameters were statistically significant (p < 0.05) between the comparison group and the dehydrated group: difference in heart rate, diastolic blood pressure, urine sodium/potassium ratio, urine sodium, fractional sodium excretion, serum bicarbonate, and creatinine measurements. The best markers for dehydration were urine Na and serum bicarbonate (ROC AUC = 0.798 and 0.821, respectively). CDS was most closely correlated with serum bicarbonate (Pearson r = -0.3696, p = 0.002).
Conclusion: Although serum bicarbonate is not the gold standard for dehydration, this study provides further evidence for the usefulness of the CDS as a dehydration marker in children.
Trial registration: Registered at ClinicalTrials.gov (NCT00462527) on April 18, 2007.
Figures
References
-
- Liebelt EL. Clinical and laboratory evaluation and management of children with vomiting, diarrhea, and dehydration. Curr Opin Pediatr. 1998;10(5):461–469. - PubMed
-
- Rothrock SG, Green SM, McArthur CL, DelDuca K. Detection of electrolyte abnormalities in children presenting to the emergency department: a multicenter, prospective analysis. Detection of Electrolyte Abnormalities in Children Observational National Study (DEACONS) Investigators. Acad Emerg Med. 1997;4(11):1025–1031. - PubMed
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, Rudan I, Campbell H, Cibulskis R, Li M, Mathers C, Black RE. Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379(9832):2151–2161. - PubMed
-
- Gorelick MH, Shaw KN, Murphy KO. Validity and reliability of clinical signs in the diagnosis of dehydration in children. Pediatrics. 1997;99(5):E6. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
