

HIV among people who inject drugs in the Middle East and North Africa: systematic review and data synthesis
- PMID: 24937136
- PMCID: PMC4061009
- DOI: 10.1371/journal.pmed.1001663
HIV among people who inject drugs in the Middle East and North Africa: systematic review and data synthesis
Abstract
Background: It is perceived that little is known about the epidemiology of HIV infection among people who inject drugs (PWID) in the Middle East and North Africa (MENA). The primary objective of this study was to assess the status of the HIV epidemic among PWID in MENA by describing HIV prevalence and incidence. Secondary objectives were to describe the risk behavior environment and the HIV epidemic potential among PWID, and to estimate the prevalence of injecting drug use in MENA.
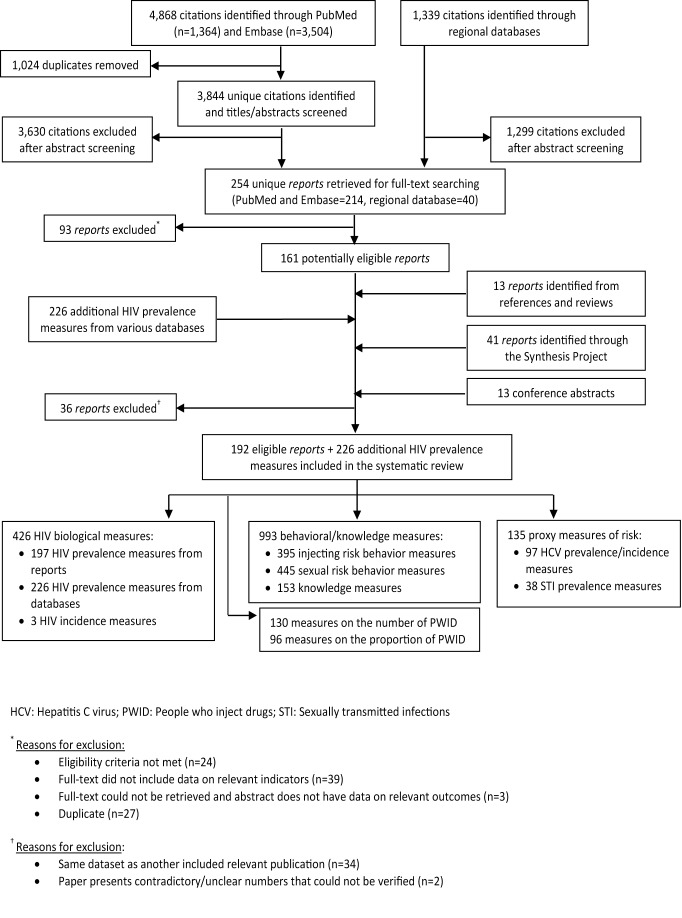
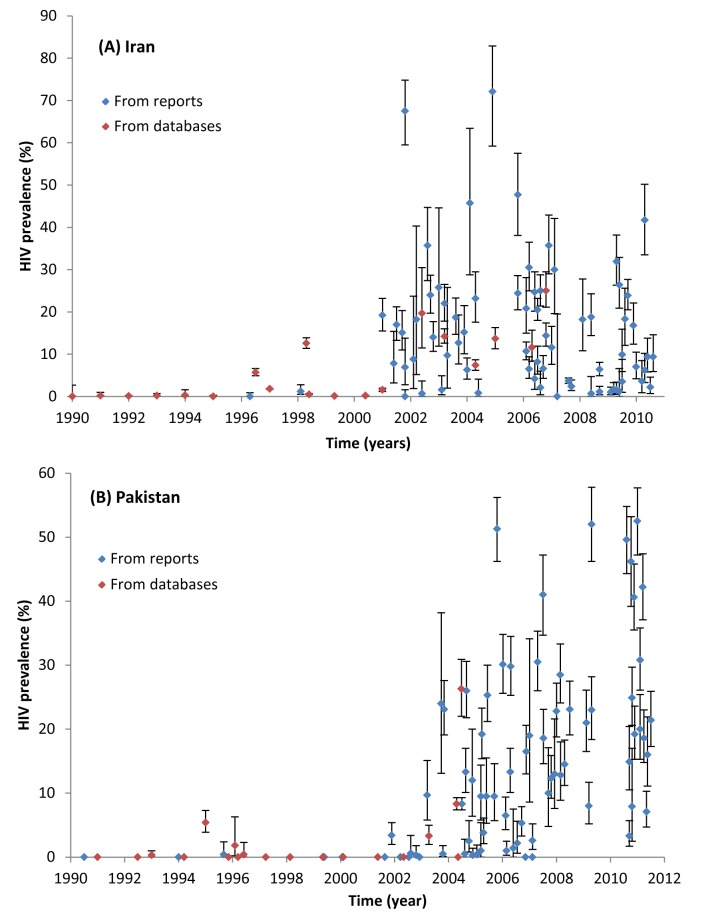
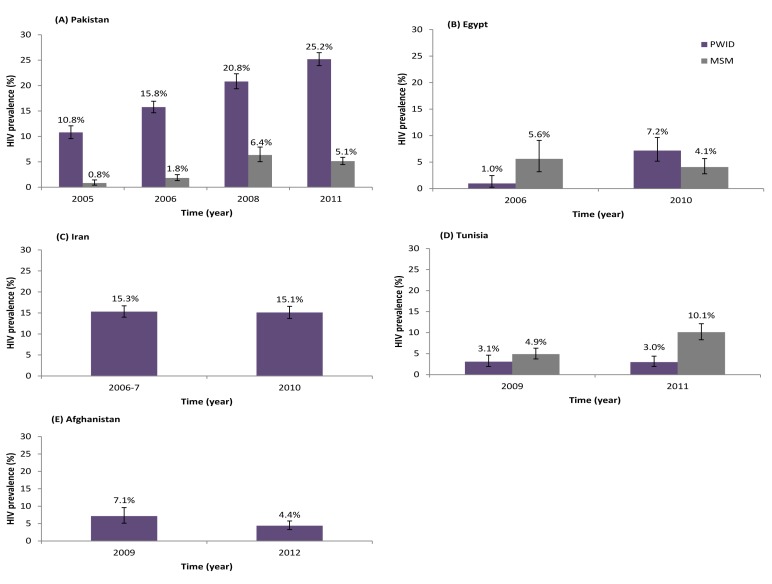
Methods and findings: This was a systematic review following the PRISMA guidelines and covering 23 MENA countries. PubMed, Embase, regional and international databases, as well as country-level reports were searched up to December 16, 2013. Primary studies reporting (1) the prevalence/incidence of HIV, other sexually transmitted infections, or hepatitis C virus (HCV) among PWIDs; or (2) the prevalence of injecting or sexual risk behaviors, or HIV knowledge among PWID; or (3) the number/proportion of PWID in MENA countries, were eligible for inclusion. The quality, quantity, and geographic coverage of the data were assessed at country level. Risk of bias in predefined quality domains was described to assess the quality of available HIV prevalence measures. After multiple level screening, 192 eligible reports were included in the review. There were 197 HIV prevalence measures on a total of 58,241 PWID extracted from reports, and an additional 226 HIV prevalence measures extracted from the databases. We estimated that there are 626,000 PWID in MENA (range: 335,000-1,635,000, prevalence of 0.24 per 100 adults). We found evidence of HIV epidemics among PWID in at least one-third of MENA countries, most of which are emerging concentrated epidemics and with HIV prevalence overall in the range of 10%-15%. Some of the epidemics have however already reached considerable levels including some of the highest HIV prevalence among PWID globally (87.1% in Tripoli, Libya). The relatively high prevalence of sharing needles/syringes (18%-28% in the last injection), the low levels of condom use (20%-54% ever condom use), the high levels of having sex with sex workers and of men having sex with men (15%-30% and 2%-10% in the last year, respectively), and of selling sex (5%-29% in the last year), indicate a high injecting and sexual risk environment. The prevalence of HCV (31%-64%) and of sexually transmitted infections suggest high levels of risk behavior indicative of the potential for more and larger HIV epidemics.
Conclusions: Our study identified a large volume of HIV-related biological and behavioral data among PWID in the MENA region. The coverage and quality of the data varied between countries. There is robust evidence for HIV epidemics among PWID in multiple countries, most of which have emerged within the last decade and continue to grow. The lack of sufficient evidence in some MENA countries does not preclude the possibility of hidden epidemics among PWID in these settings. With the HIV epidemic among PWID in overall a relatively early phase, there is a window of opportunity for prevention that should not be missed through the provision of comprehensive programs, including scale-up of harm reduction services and expansion of surveillance systems.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- UNAIDS (2010) Global Report: UNAIDS report on the global AIDS epidemic. Available: http://www.unaids.org/documents/20101123_GlobalReport_em.pdf. Accessed 16 May 2014.
-
- Aceijas C, Stimson GV, Hickman M, Rhodes T (2004) Global overview of injecting drug use and HIV infection among injecting drug users. AIDS 18: 2295–2303. - PubMed
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ (2006) Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet 367: 1747–1757. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
