

Pseudomonas aeruginosa in vitro phenotypes distinguish cystic fibrosis infection stages and outcomes
- PMID: 24937177
- PMCID: PMC4226041
- DOI: 10.1164/rccm.201404-0681OC
Pseudomonas aeruginosa in vitro phenotypes distinguish cystic fibrosis infection stages and outcomes
Abstract
Rationale: Pseudomonas aeruginosa undergoes phenotypic changes during cystic fibrosis (CF) lung infection. Although mucoidy is traditionally associated with transition to chronic infection, we hypothesized that additional in vitro phenotypes correlate with this transition and contribute to disease.
Objectives: To characterize the relationships between in vitro P. aeruginosa phenotypes, infection stage, and clinical outcomes.
Methods: A total of 649 children with CF and newly identified P. aeruginosa were followed for a median 5.4 years during which a total of 2,594 P. aeruginosa isolates were collected. Twenty-six in vitro bacterial phenotypes were assessed among the isolates, including measures of motility, exoproduct production, colony morphology, growth, and metabolism.
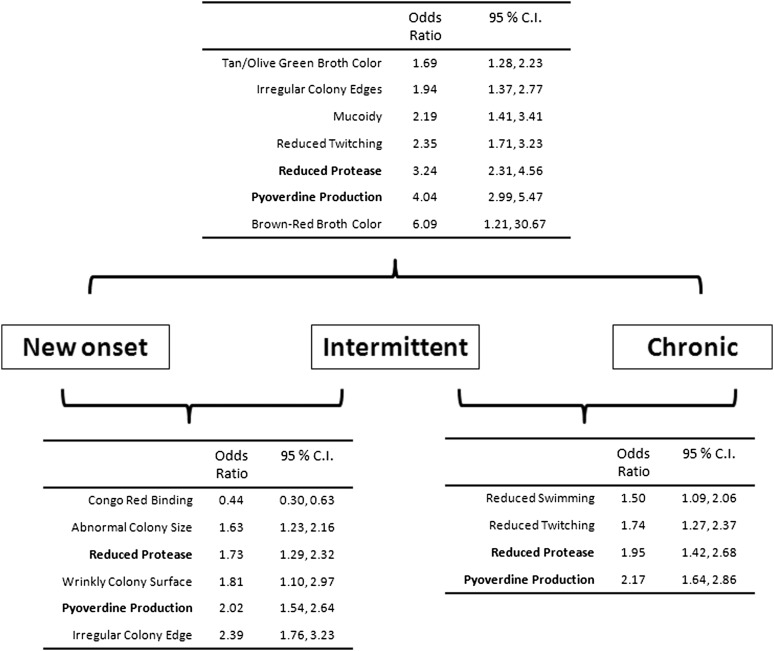
Measurements and main results: P. aeruginosa phenotypes present at the time of culture were associated with both stage of infection (new onset, intermittent, or chronic) and the primary clinical outcome, occurrence of a pulmonary exacerbation (PE) in the subsequent 2 years. Two in vitro P. aeruginosa phenotypes best distinguished infection stages: pyoverdine production (31% of new-onset cultures, 48% of intermittent, 69% of chronic) and reduced protease production (31%, 39%, and 65%, respectively). The best P. aeruginosa phenotypic predictors of subsequent occurrence of a PE were mucoidy (odds ratio, 1.75; 95% confidence interval, 1.19-2.57) and reduced twitching motility (odds ratio, 1.43; 95% confidence interval, 1.11-1.84).
Conclusions: In this large epidemiologic study of CF P. aeruginosa adaptation, P. aeruginosa isolates exhibited two in vitro phenotypes that best distinguished early and later infection stages. Among the many phenotypes tested, mucoidy and reduced twitching best predicted subsequent PE. These phenotypes indicate potentially useful prognostic markers of transition to chronic infection and advancing lung disease.
Keywords: epidemiology; exacerbation; mucoid Pseudomonas aeruginosa; pulmonary function; risk factors.
Figures

Comment in
-
Phenotypes that matter: Pseudomonas aeruginosa and progression of cystic fibrosis lung disease.Am J Respir Crit Care Med. 2014 Aug 1;190(3):245-6. doi: 10.1164/rccm.201406-1145ED. Am J Respir Crit Care Med. 2014. PMID: 25084257 No abstract available.
References
-
- Gibson RL, Burns JL, Ramsey BW. Pathophysiology and management of pulmonary infections in cystic fibrosis. Am J Respir Crit Care Med. 2003;168:918–951. - PubMed
-
- Henry RL, Mellis CM, Petrovic L. Mucoid Pseudomonas aeruginosa is a marker of poor survival in cystic fibrosis. Pediatr Pulmonol. 1992;12:158–161. - PubMed
-
- Pamukcu A, Bush A, Buchdahl R. Effects of Pseudomonas aeruginosa colonization on lung function and anthropometric variables in children with cystic fibrosis. Pediatr Pulmonol. 1995;19:10–15. - PubMed
-
- Rabin HR, Butler SM, Wohl ME, Geller DE, Colin AA, Schidlow DV, Johnson CA, Konstan MW, Regelmann WE. Pulmonary exacerbations in cystic fibrosis. Pediatr Pulmonol. 2004;37:400–406. - PubMed
-
- Kerem E, Corey M, Gold R, Levison H. Pulmonary function and clinical course in patients with cystic fibrosis after pulmonary colonization with Pseudomonas aeruginosa. J Pediatr. 1990;116:714–719. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
