

Bosentan in pulmonary hypertension associated with fibrotic idiopathic interstitial pneumonia
- PMID: 24937643
- PMCID: PMC4226056
- DOI: 10.1164/rccm.201403-0446OC
Bosentan in pulmonary hypertension associated with fibrotic idiopathic interstitial pneumonia
Abstract
Rationale: Pulmonary hypertension (PH) associated with fibrotic idiopathic interstitial pneumonia (IIP; idiopathic pulmonary fibrosis and nonspecific interstitial pneumonia) confers important additional morbidity and mortality.
Objectives: To evaluate the safety and clinical efficacy of the dual endothelin-1 receptor antagonist bosentan in this patient group.
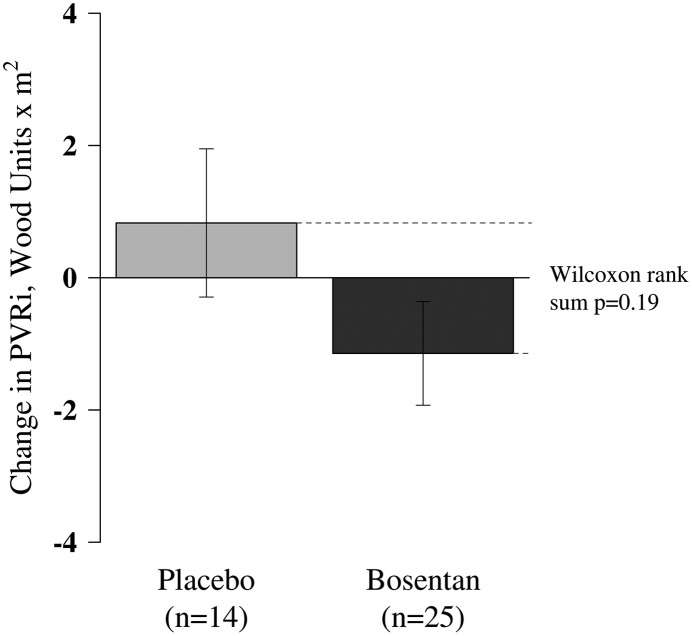
Methods: In a randomized, double-blind, placebo-controlled study, 60 patients with fibrotic IIP and right heart catheter confirmed PH were randomized 2:1 to bosentan (n = 40) or placebo (n = 20). The primary study endpoint was a fall from baseline pulmonary vascular resistance index (PVRi) of 20% or more over 16 weeks.
Measurements and main results: Sixty patients (42 men; mean age, 66.6 ± 9.2 yr), with a mean pulmonary artery pressure of 36.0 (± 8.9) mm Hg, PVRi 13.0 (± 6.7) Wood Units/m(2) and reduced cardiac index of 2.21 (± 0.5) L/min/m(2) were recruited to the study. Accounting for deaths and withdrawals, paired right heart catheter data were available for analysis in 39 patients (bosentan = 25, placebo = 14). No difference in the primary outcome was detected, with seven (28.0%) patients receiving bosentan, and four (28.6%) receiving placebo achieving a reduction in PVRi of greater than or equal to 20% (P = 0.97) at 16 weeks. There was no change in functional capacity or symptoms between the two groups at 16 weeks, nor any difference in rates of serious adverse events or deaths (three deaths in each group).
Conclusions: This study shows no difference in invasive pulmonary hemodynamics, functional capacity, or symptoms between the bosentan and placebo groups over 16 weeks. Our data do not support the use of the dual endothelin-1 receptor antagonist, bosentan, in patients with PH and fibrotic IIP. Clinical trial registered with www.clinicaltrials.gov (NCT 00637065).
Trial registration: ClinicalTrials.gov NCT00637065.
Keywords: clinical trial; hypertension; interstitial lung diseases; pulmonary.
Figures



Comment in
-
Pulmonary hypertension due to fibrotic lung disease: hidden value in a neutral trial.Am J Respir Crit Care Med. 2014 Jul 15;190(2):131-2. doi: 10.1164/rccm.201406-1094ED. Am J Respir Crit Care Med. 2014. PMID: 25025352 No abstract available.
References
-
- Minai OA, Santacruz JF, Alster JM, Budev MM, McCarthy K. Impact of pulmonary hemodynamics on 6-min walk test in idiopathic pulmonary fibrosis. Respir Med. 2012;106:1613–1621. - PubMed
-
- Lettieri CJ, Nathan SD, Barnett SD, Ahmad S, Shorr AF. Prevalence and outcomes of pulmonary arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest. 2006;129:746–752. - PubMed
-
- Shorr AF, Wainright JL, Cors CS, Lettieri CJ, Nathan SD. Pulmonary hypertension in patients with pulmonary fibrosis awaiting lung transplant. Eur Respir J. 2007;30:715–721. - PubMed
-
- Yang SJ, Hoffman C, Mulligan K.Pulmonary arterial hypertension in patients with idiopathic pulmonary fibrosis when listed for lung transplantation Proc Am Thorac Soc 20063:A369
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
